


ORIGINAL ARTICLES
Introduction. The most widely used operative technique for distal hypospadias is tubularized incised plate (TIP) urethroplasty. Despite its relative technical simplicity and favourable outcomes, TIP may be complicated by scarring of the distal urethra, meatal stenosis and urethrocutaneous fistulae, which may be related to a small glans and a narrow urethral plate. A grafted TIP (Grafted-TIP) modification has been proposed to address these issues; however, clear indications for its use in primary urethroplasty for distal hypospadias in children are lacking in the literature.
Objective. To assess the variability of urethral meatal anatomy and its impact on postoperative outcomes in boys undergoing repair of distal hypospadias.
Materials & methods. Between 2021 and 2022, 43 boys aged 10 months to 8 years underwent primary repair of distal hypospadias using the TIP technique. Intraoperative measurements of glans and urethral meatus dimensions were obtained with a calliper and ruler, recorded in a standardized datasheet, and subjected to subsequent statistical analysis. Based on published data on normal meatal anatomy in healthy boys (vertical meatal length 5.4 ± 1.0 mm), patients were stratified into two groups according to meatal size: group 1, meatal length < 0.05). The mean urinary flow rate was also higher in group 1, meatal length <5 mm; group 2, meatal
length ≥5 mm. Postoperative assessments were performed at 3 and 12 months and included cosmetic appearance, meatal position and size, and voiding parameters.
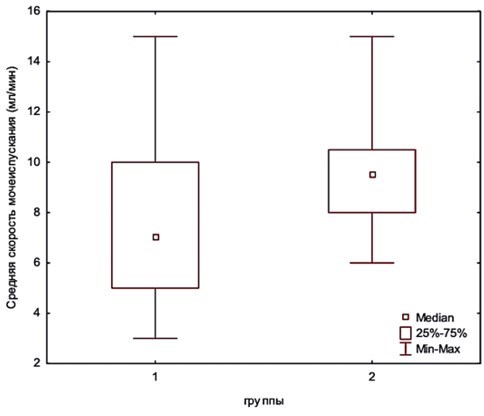
Results. The mean urethral plate width was significantly greater in group 2 than in group 1 (8.5 ± 1.7 vs 5.6 ± 2.6 mm, p< 0.05). The mean urinary flow rate was also higher in group 2 compared with group 1 (9.4 ± 2.1 vs 7.8 ± 3.3 ml/s). Postoperative complications were more frequent in group 1, although the difference was not statistically significant; the fistula rate was similar between groups, whereas no cases of wound dehiscence or cicatricial meatal stenosis occurred in group 2. HOPE score analysis showed no statistically significant difference between the groups (p > 0.05).
Conclusion. A vertical meatal length of 5 mm or greater appears to allow creation of a neomeatus comparable in size to that of healthy boys. This threshold is associated with a statistically significant improvement in urinary dynamics, reflected by higher mean urinary flow rates. Continued follow-up of this cohort will facilitate further evaluation of how anatomical characteristics of the penis in hypospadias influence long-term surgical outcomes.
Introduction. Prostate cancer remains one of the leading oncological diseases among men, necessitating precise diagnostic strategies. Contemporary approaches, including multiparametric MRI (mpMRI) with PI-RADS scoring and targeted biopsy, enhance detection of clinically significant prostate cancer (csPCa), reduce unnecessary procedures, and minimize complications.
Objective. To evaluate the efficacy of transrectal mpMRI/transrectal ultrasound (TRUS) fusion-guided prostate biopsy in detecting csPCa.
Materials & methods. We prospectively evaluated 318 patients who underwent transrectal mpMRI/TRUS fusion-guided prostate biopsy. All patients had pre-biopsy mpMRI with PI-RADS scoring, prostate-specific antigen (PSA) levels, PSA density, and digital rectal examination (DRE). Biopsies employed a combined approach: targeted sampling of mpMRIidentified lesions plus systematic sampling. Prostate cancer detection rates (csPCa defined as ISUP grade ≥ 2) were correlated with PI-RADS score, PSA density, and DRE findings. Detection rates were compared between biopsy-naïve and repeat-biopsy patients. Complications were systematically recorded.
Results. csPCa was detected in 40% of patients overall (43% in biopsy-naïve vs. 35% in repeat-biopsy patients; p > 0.05). Lesions scored PI-RADS 4 – 5 yielded significantly higher csPCa detection rates than PI-RADS 3 lesions. Among PI-RADS 3 cases, PSA density > 0.15 ng/mL/cm³ predicted higher csPCa risk, while lower values indicated low risk. Positive DRE also correlated with csPCa detection. Targeted biopsy detected most csPCa cases, but systematic sampling increased the overall yield by 10%. No severe complications (e.g., sepsis or major hemorrhage) occurred; minor, transient events such as hematuria or fever affected < 5% of patients.
Conclusions. Transrectal mpMRI/TRUS fusion-guided biopsy is highly effective for csPCa detection. Pre-biopsy mpMRI combined with targeted plus systematic sampling optimizes diagnostic yield while maintaining a favorable safety profile.
Introduction. The principal aim of surgery for urethral stricture is to restore satisfactory voiding. Given the refinement and standardisation of contemporary reconstructive techniques, excellent functional urinary outcomes are now routinely achievable. Nevertheless, men of reproductive and middle age are often equally concerned about preserving fertility. Currently, however, the literature provides very limited information on reproductive outcomes in men following urethroplasty.
Objective. To characterise the pattern and prevalence of reproductive disorders in men who have undergone surgical treatment for urethral stricture.
Materials & methods. In this prospective comparative cohort study, 54 men were enrolled: 30 patients with anterior urethral stricture who underwent urethroplasty and 24 men who had circumcision and served as a comparison group. In addition to standard preoperative assessment, all participants underwent semen analysis, measurement of serum hormones (total testosterone, LH, FSH), scrotal ultrasonography, and transrectal ultrasound of the prostate and seminal vesicles. These investigations were performed preoperatively and then repeated at 3, 6 and 12 months after surgery.
Results. Comparison of baseline characteristics between groups showed statistically significant differences in semen analysis parameters and ultrasound findings, but not in hormonal profile, with FSH, LH and total testosterone levels remaining comparable. At three months after urethroplasty there was an increase in the prevalence of signs of male accessory gland inflammation (from 40.0% to 63.3%), leukocytospermia (from 20.0% to 46.7%) and abnormal semen viscosity (from 33.3% to 53.3%). In addition, the proportion of positive semen cultures rose from 33.3% to 53.3% in the urethral reconstruction group.
Conclusion. Statistically significant postoperative changes included higher rates of abnormal semen viscosity, leukocytospermia and altered ejaculate pH. Furthermore, men after urethroplasty showed an increased frequency of male accessory gland inflammation.
Introduction. Urethral stricture is a common urological condition that substantially impairs patients' quality of life. Historically, restoration of spontaneous voiding has been considered the primary success criterion for stricture management. However, contemporary urethroplasty decision-making rarely accounts for potential postoperative sexual dysfunctions in men, including ejaculatory and erectile disorders, penile curvature and shortening, reduced genital sensation, and impaired glans blood supply.
Objective. To identify risk factors for ejaculatory dysfunction following urethroplasty and quantify their impact.
Materials & methods. We evaluated 74 patients with urethral strictures treated surgically from 2015 to 2024. Ejaculatory function was assessed using the Male Sexual Health Questionnaire — Ejaculatory Dysfunction Short Form (MSHQ-EjD SF) preoperatively and at 12 months postoperatively.
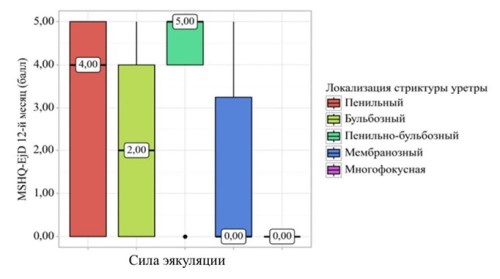
Results. At 12 months, patients aged ≥ 60 years exhibited statistically significant declines in ejaculation achievement, force, and ejaculate volume. Similar deteriorations occurred in patients with hypertension and diabetes mellitus (across all three parameters) and coronary artery disease (ejaculation force and volume only). Conversely, patients undergoing urethroplasty without corpus spongiosum transection showed preserved ejaculation parameters.
Conclusion. Urethroplasty may induce de novo ejaculatory dysfunction. Principal risk factors include advanced age (≥ 60 years), comorbidities (hypertension, diabetes mellitus, coronary artery disease), and surgical transection of the corpus spongiosum.
Introduction. Varicocele is a well-characterized cause of spermatogenic impairment with established mechanisms of testicular tissue damage. Among antioxidants, L-carnitine is the most extensively studied agent for mitigating oxidative stress, optimizing sperm metabolism, maturation, and motility. However, available clinical literature presents conflicting data on the effects of carnitine supplementation on semen parameters.
Objective. To evaluate the impact of L-carnitine on semen analysis parameters in an experimental chronic varicocele model.
Materials & methods. Fifteen male rabbits were randomized into three groups: Group 1 (intact controls, n = 5); Group 2 (varicocele model without treatment, sacrificed at one-month post-induction, n = 5); Group 3 (varicocele model with L-carnitine treatment for one-month post-induction, n = 5). Varicocele was induced by partial ligation (50 – 67% narrowing) of the left renal vein, combined with daily gonadotropin (300 IU/kg) and 0.2 mL of 1% progesterone solution for 10 days starting 24 hours prior to ligation. L-carnitine was administered intragastrically at 26.15 mg/day (adjusted for rabbit metabolic differences) in Group 3. Semen was analyzed by light microscopy, assessing sperm count and quality.
Results. At 14 days post-induction, seminal veins were visible (up to 1.8 mm diameter, no intergroup differences) with confirmed reflux. Mean vein diameter reached 2.1 mm by day 30. Left testis volume progressively declined by 0.6 cm³ (from 0.77 to 0.71 cm³) over 30 days (p > 0.05 across groups). Baseline semen parameters in Group 1 were significantly superior to Groups 2 and 3 (p < 0.05 – 0.01). Total sperm count was 310.2 million (Group 1), 199.3 million (Group 2), and 247.6 million (Group 3). Group 2 parameters were significantly inferior to Group 3: total sperm count (199.3 vs 247.6 million), live forms (68.3% vs 80.6%), PR+NP (61.5% vs 73.4%), PR (48.7% vs 65.4%), and sperm velocity (4 vs 8 μm/s) (p < 0.01).
Conclusions. In a chronic varicocele model with persistent injurious stimulus, L-carnitine supplementation significantly improved both quantitative and qualitative semen parameters.
Introduction. Urolithiasis represents a major urological challenge, affecting 10 – 15% of the population with recurrence rates of 30 – 50%. Transurethral nephrolithotripsy (TUNL) is a contemporary approach for stones ≤ 2 cm. The adoption of aspiration ureteral access sheaths enables vacuum-assisted fragment evacuation, enhancing treatment outcomes by reducing operative time and minimising infectious complications.
Objective. To evaluate the clinical efficacy and safety of aspiration sheaths during TUNL compared with standard sheaths.
Materials & methods. This prospective randomised study enrolled 32 patients with nephrolithiasis, randomised 1:1 to two groups (n = 16 each). Group 1 underwent TUNL using a 12/14 Fr aspiration sheath (ClearPetra®); group 2 received a standard 12/14 Fr ureteral access sheath (Navigator™ HD, Boston Scientific). Patient demographics, stone characteristics, and intra-/postoperative outcomes were prospectively collected and analysed.
Results. Operative and lithotripsy times were shorter in group 1. Stone-free rate (SFR) was 93.8% (group 1) versus 81.3% (group 2). Postoperative leucocytosis and C-reactive protein rises were less pronounced in group 1 (9 ± 1.3 and 5.5 ± 1.1, respectively) than group 2 (10.4 ± 2.3 and 7.9 ± 2.1). Hospital stay was shorter in group 1 (2.0 ± 0.5 days) versus group 2 (4.0 ± 0.6 days).
Conclusion. Aspiration ureteral access sheaths during TUNL offer a safe, efficacious option for renal stones ≤ 2 cm, yielding superior SFR, reduced infectious risk, and shorter hospitalisation compared with standard sheaths.
Introduction. Cytoreductive nephrectomy (CN) remains the standard of care in multimodal treatment for metastatic renal cell carcinoma (mRCC) with favorable prognosis. Cytoreductive partial nephrectomy (CPN), however, is infrequently performed in mRCC.
Objective. To compare the effectiveness of CPN versus CN in real-world clinical practice.
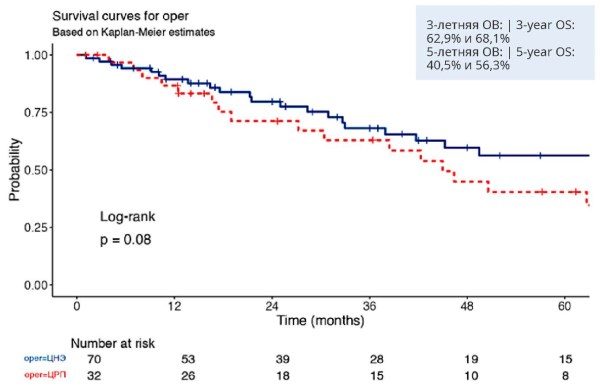
Materials & methods. This retrospective study included 102 patients with mRCC, comprising 32 who underwent CPN and 70 who underwent CN. Disease outcomes encompassed all-cause mortality, 30-day mortality, and 90-day mortality, stratified by cytoreductive surgery type (CPN vs CN). Clinical data were retrospectively retrieved and analyzed from medical records, with all patients undergoing comprehensive clinical-laboratory and histopathological evaluation. The primary endpoint was overall survival (OS) in patients undergoing CPN or CN. Secondary outcomes included length of hospital stay and readmission rates. Survival metrics were assessed using survival analysis, including life tables and Kaplan-Meier curves.
Results. Compared to the CN group, patients undergoing CPN less frequently had clear cell RCC (84.4% vs 97.1%), poorly differentiated tumors (21.9% vs 41.4%), synchronous metastases (21.9% vs 40.0%), and multiple metastases (59.4% vs 78.6%). Clinical T1 stage was significantly more common in the CPN group (84.4% vs 15.8%). CPN patients more often belonged to the favorable IMDC prognostic group (34.4% vs 25.7%). Lung metastases (53.1% vs 80.0%) and lymph node involvement (6.2% vs 22.8%) were less frequent in the CPN cohort, as were checkpoint inhibitor therapies (3.1% vs 18.6%) and radiotherapy (6.2% vs 18.6%). Three- and five-year OS rates were 62.9% and 40.5% for CPN versus 68.1% and 56.3% for CN, respectively (p = 0.08).
Conclusions. Optimal indications for cytoreductive partial nephrectomy in mRCC remain undefined. Despite more favorable baseline characteristics in the CPN cohort, overall survival favored the CN group. Further research is needed to identify patients most suitable for this palliative approach, aiming to refine personalized treatment strategies and improve survival outcomes.
Introduction. Radical cystectomy (RC) effectively controls bladder cancer but carries a > 50% 90-day complication rate, 15 – 20% severe complications, and 2% mortality. Most short- and long-term complications relate to urinary diversion rather than RC itself.
Objective. To evaluate the incidence and profile of delayed postoperative complications following RC by urinary diversion method in non-muscle-invasive bladder cancer (NMIBC) and minimal intradetrusor-invasive muscle-invasive bladder cancer (MIBC).
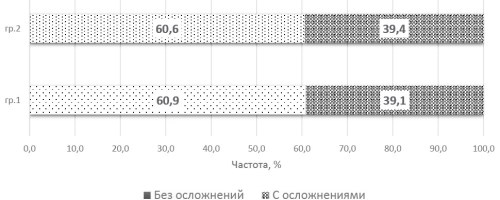
Materials & methods. This study included 49 patients with high-risk progressive NMIBC (group 1) and 102 with MIBC exhibiting minimal intradetrusor invasion (group 2) who underwent RC.
Results. Delayed complications occurred in 10.9 ± 4.9 (group 1) versus 12.1 ± 3.5 cases per 100 patients (group 2; no significant difference). Diversion-related complications were 5.5 times more frequent than non-diversion-related ones. Proportions of affected patients were similar (39.1% vs 39.4%), but case prevalence was higher in group 2 (71.7 ± 8.5 vs 60.9 ± 11.5 per 100; p > 0.05). Internal diversion showed the highest risk (266.7 ± 66.7 per 100), while inverted ileocystoplasty was most favourable (34.8 ± 12.3 per 100). Bricker diversion had the lowest corrective surgery rate (6.3 ± 4.4 per 100).
Conclusion. Delayed diversion-related and urological complications were more prevalent in minimal MIBC, with higher corrective surgeries in NMIBC. Internal diversion performed poorly, whereas orthotopic inverted ileocystoplasty offered optimal outcomes.
REVIEWS ARTICLE
Introduction. Artificial intelligence (AI) is becoming a key tool in modern medicine, enhancing diagnostic accuracy, treatment personalization, and patient management. In urogynecology, the integration of AI opens new opportunities for improving medical image interpretation, urodynamic data analysis, outcome prediction, and remote patient monitoring.
Objective. To systematize current evidence on the use of AI technologies in urogynecology, assess their diagnostic and prognostic potential, and outline prospects for their implementation in clinical practice.
Materials & methods. A comprehensive search and analysis of Russian and international publications were conducted in eLIBRARY, PubMed, Scopus, and Web of Science databases for the period 2020–2025 using the keywords: urogynecology, female urology, artificial intelligence, machine learning. Studies describing the use of AI in diagnostics, treatment, prognosis, and patient monitoring were included.
Results. AI is actively applied for analyzing electronic medical records, interpreting urodynamic tests, and segmenting ultrasound and MRI images, thereby improving the accuracy of diagnosing pelvic organ prolapse and urinary incontinence. In surgical practice, computer vision and augmented reality technologies enhance the precision and safety of operations. Predictive algorithms enable assessment of postoperative complications and recurrence risks, while telemedicine and wearable AI-based systems provide continuous patient monitoring. Despite their promising potential, most models still require additional clinical validation and standardization.
Conclusions. The use of AI in urogynecology contributes to improved diagnostic accuracy, personalized treatment, and better clinical outcomes. Broader implementation requires multicenter studies, further algorithm development, and the establishment of ethical and legal frameworks for AI integration into medical practice.
Vesicoureteral reflux (VUR) is a common condition in paediatric urology that increases the risk of urinary tract infection (UTI), which in turn may result in renal scarring and the development of chronic kidney disease in children. A first episode of UTI is often the trigger for the diagnosis of VUR. Antibiotic therapy remains the mainstay of UTI management, while continuous antibiotic prophylaxis is used to prevent recurrence and infectious complications in children with VUR. However, prolonged antibiotic use is associated with important risks, including the development of antimicrobial resistance. This review evaluates the efficacy and safety of contemporary antibiotic treatment and prophylactic strategies in children with VUR. Particular emphasis is placed on optimizing patient management and on current guideline-based recommendations aimed at reducing recurrence rates and improving clinical outcomes.
EXCHANGE OF PRACTICAL EXPERIENCE
Introduction. Division of the penile suspensory ligament (ligamentotomy) is a surgical procedure aimed at lengthening the visible part of the penis. This operation is widely used in aesthetic and reconstructive surgery for patients who are dissatisfied with the size of their penis or suffer from psychosexual discomfort. As with any surgical treatment, ligamentotomy also carries risks of complications.
Objective. To evaluate the frequency and structure of postoperative complications in patients who have undergone penile suspensory ligament division.
Materials & methods. We analyzed the frequency and type of complications in 66 patients who underwent division of the suspensory ligament of the penis in combination with various skin plasty techniques.
Results. The most common complications in this cohort of patients are seroma, penile edema, gross scarring, and superficial wound complications. Complications were mainly classified as grade I and II according to the ClavienDindo classification.
Conclusions. Serious complications are rare during ligamentotomy. Mild and moderate conditions predominate, requiring no additional surgical interventions. The Clavien–Dindo classification allows for objective risk stratification and may be recommended for use in clinical practice when assessing the outcomes of penile augmentation surgery.
Introduction. Cryptorchidism is a common congenital anomaly in which the testes fail to descend normally into the scrotum. Although most cases can be corrected surgically, some patients miss the optimal window for treatment and, as they grow, may present with acute complications such as testicular torsion.
Objective. To analyse our experience with the diagnosis and treatment outcomes of testicular torsion in children with cryptorchidism.
Materials & methods. We retrospectively reviewed clinical data from 7 boys with cryptorchidism who developed testicular torsion and underwent surgical treatment at the Chelyabinsk Regional Children’s Hospital between 2018 and 2024. Preoperative scrotal ultrasonography was performed in all cases. Postoperative follow‑up was 12 months.
Results. The mean age at presentation was 48 months. Testicular torsion involved the left side in 5 cases and the right side in 2 cases, with the degree of twisting ranging from 360° to 720°. The median interval between symptom onset and surgery was 24 hours, and the mean operative time was 25 minutes. Irreversible testicular necrosis was found in 5 patients, who underwent orchiectomy, whereas in 2 patients the testes were successfully detorsed and preserved with good intraoperative perfusion. During follow‑up, testicular atrophy developed in 1 preserved testis. In children who underwent orchiectomy, the contralateral fixed testes showed normal development.
Conclusion. Testicular torsion in children with cryptorchidism is rare and often presents with subtle symptoms, making early recognition challenging. Prompt diagnosis and treatment are crucial for testicular salvage. Ultrasonography plays an important role in the diagnosis of testicular torsion in the setting of cryptorchidism.

Introduction. Partial nephrectomy is the gold‑standard treatment for localised renal cell carcinoma. Further gains in outcomes after nephron‑sparing surgery require a shift in treatment strategy, with management centred on optimising the technique of partial nephrectomy so as to preserve the greatest possible number of functioning nephrons.
Objective. To develop an in-practice algorithm for robot‑assisted nephron‑sparing partial nephrectomy and to report early clinical outcomes following its implementation.
Materials & methods. We outline the core principles underpinning nephron‑sparing surgery and provide a detailed, stepwise description of the operative workflow for partial nephrectomy. Technical considerations are discussed in relation to case complexity. We reviewed the first 100 nephron‑sparing procedures performed at the Botkin Moscow Multidisciplinary Clinical Research Centre between 2020 and 2021 (70 laparoscopic and 30 robot‑assisted partial nephrectomies) within a prospective cohort, with renal functional outcomes assessed at one year postoperatively.
Results. Preoperatively, most patients had clinical stage cT1a disease (n=70), with cT1b (n=14) and cT2 (n=4) tumours comprising the remainder; cystic renal lesions were present in 12 patients. Warm ischaemia was applied in 14% of cases, with a mean duration of 9 minutes and a maximum duration of 25 minutes. The negative surgical margin rate was 97%. Trifecta outcomes were achieved in 89% of patients, while Pentafecta criteria were met in 55%.
Conclusion. Adherence to nephron‑sparing surgical principles can enhance functional outcomes following organ‑preserving renal surgery. The detailed operative algorithm presented here may be particularly useful when establishing a minimally invasive partial nephrectomy programme.
CURRENT STATE-OF-THE-ART
In accordance with contemporary clinical guidelines, intravesical BCG immunotherapy is indicated for patients with intermediate‑ and high‑risk non‑muscle‑invasive bladder cancer (NMIBC). Nonetheless, its use is constrained by a considerable burden of adverse events, notably urogenital tuberculosis. This study therefore sought to synthesise current evidence on the most observed complications of intravesical BCG therapy, approaches to reducing treatment‑related toxicity, and structured algorithms for the management of BCG‑associated adverse events.








































