


DISCUSSION PAGE
The problem of iatrogeny, recognised even by healers of the ancient world, remains pertinent to this day. As in earlier times, addressing issues of iatrogeny is not solely the responsibility of medical professionals: law enforcement bodies supervise the proper conduct of diagnostic, therapeutic, preventive, and rehabilitative procedures. The occurrence of iatrogeny in a patient provides legitimate grounds for seeking legal recourse. Nonetheless, the broadly construed definition of iatrogeny, as developed by WHO experts, is accompanied by an almost complete lack of clear, reliable criteria to differentiate between iatrogenic and non-iatrogenic outcomes of medical interventions. Our objective in preparing this publication was to bring to the attention of specialists the concept of medico-technogenic pathology – an idea proposed roughly twenty-five years ago but undervalued and unjustly neglected – offered here as a framework for more precise medico-legal analysis of the causes, mechanisms, and consequences of iatrogeny.
ORIGINAL ARTICLES
Introduction. Infectious and inflammatory complications (ICs) are a significant, potentially life-threatening condition developing during transurethral resection of the prostate (TURP) with a frequency of 0.5% to 20.0% of cases. Most studies provide data on immediate ICs. However, there are currently no studies in the literature with a comprehensive assessment of late ICs after TURP.
Objective. To analyse the significant predictors of ICs for the development of a prognostic model for the risks of developing remote infectious complications TURP.
Materials & methods. This single-center retrospective study includes data from 301 patients who underwent monoand bipolar TURP from 2016 to 2023. Inclusion criteria for the study: prostate volume (30–80 cc), no history of urinary tract infections (UTI) at the time of hospitalization and treatment with antibacterial drugs for at least one month before surgery, possible presence of latent UTI before surgery, absence of prostate cancer. The exclusion criterion was non-compliance with the inclusion criteria. The infectious complications assessed included upper and lower urinary tract infections, as well as epididymitis, orchitis and prostatitis, confirmed based on clinical and laboratory data.
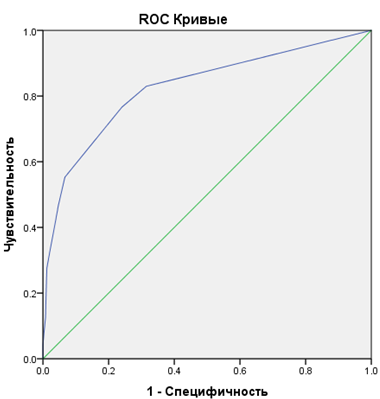
Results. In the late period, 47 (15.6%) patients developed infectious and inflammatory complications: urethritis developed in 8 cases, epididymoorchitis in 18, acute prostatitis in 9, and cystitis was diagnosed in the remaining 12 cases. Regression analysis revealed three statistically significant predictors: baseline PSA density, dysuria at hospital discharge, and scrotal discomfort / pain during hospitalization. The explained variance in the incidence of late ICs was 37.4%; the area under the curve in ROC analysis was 0.83; 95% CI [0.75; 0.90].
Conclusion. Implementation of the developed predictive model into clinical practice can improve the safety of transurethral surgery for BPH, optimize resource allocation, and improve the effectiveness of clinical outcomes in the treatment of urological infections. The predictive model can be used when discharging a patient from the hospital after TURP.
Introduction. Chronic abacterial prostatitis (CAP) / category III according to the classification of the American National Institute of Health (NIH-NIDDK USA, 1995), is diagnosed in the majority of patients with prostatitis and according to the data of a number of publications can reach 95%, which together with epidemiologic data of 10 – 45% in the population makes this problem socially significant.
Objective. To evaluate the clinical efficacy of different modes of shock wave therapy (SWT) in patients with CAP.
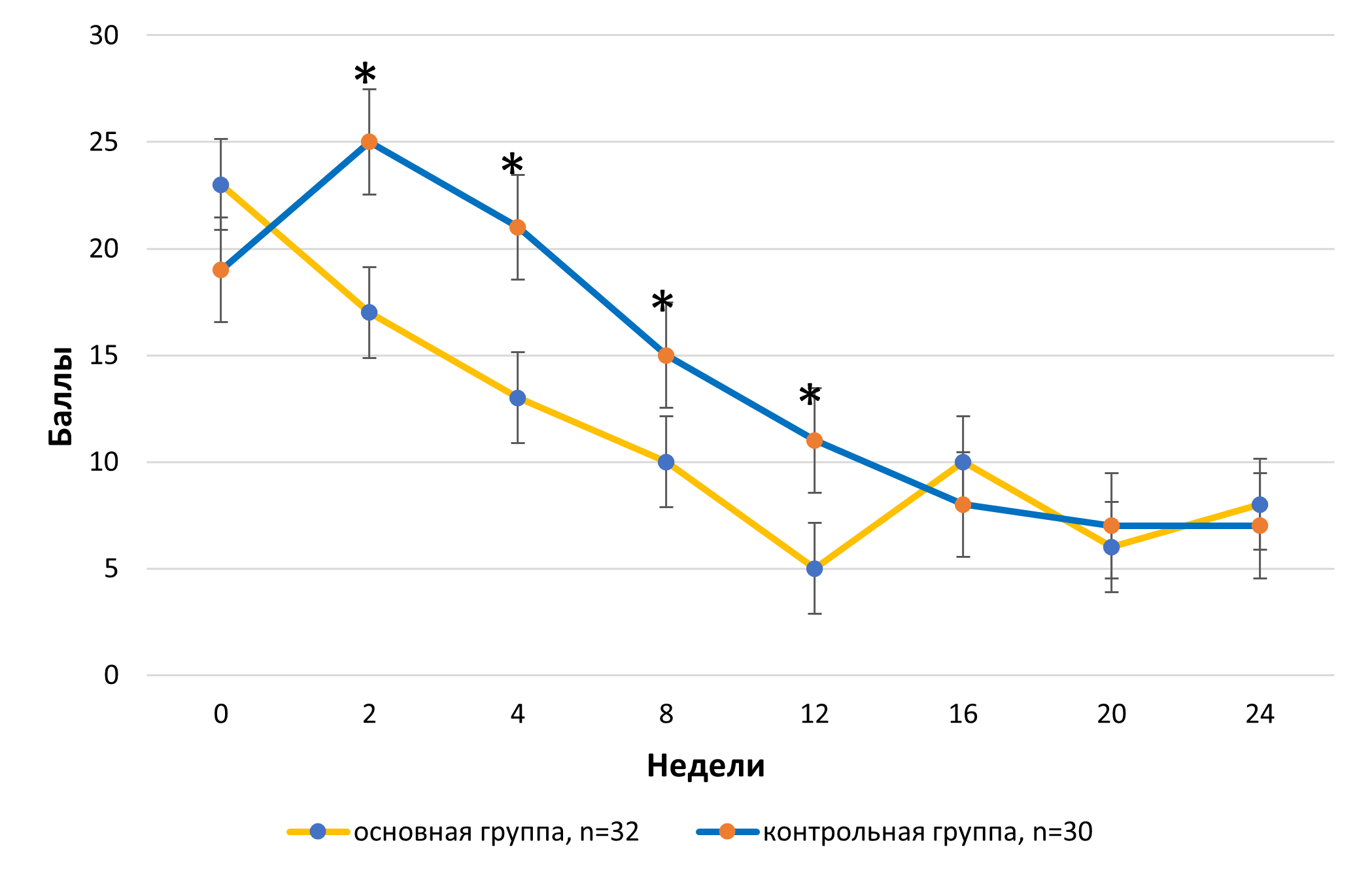
Materials & methods. We analyzed the dynamics of LUTS and pain syndrome used the IPSS and NIH-CPSI in 62 patients with CAP. Patients received standard therapy of CAP and were randomized according to the technique of SWT into control (n = 30, 12 sessions of SWT once a week according to the standard technique) and main (n = 32, SWT 36 sessions 3 times a week by fractionation up to 1/3 of the maximum pulse energy) groups. There were no differences in age, prostate volume, uroflowmetric data and symptomatology assessed by IPSS, IIEF5, LANNS, NIHCPSI, urinary diary (p > 0.05). Clinical dynamics was evaluated at 2, 4, 8, 12, 16, 20 and 24 weeks, i.e. for 12 weeks on the background and 12 weeks after treatment. Differences were considered reliable when the probability of occurrence was more than 95%.
Results. Patients of both groups before the start of therapy had clinically pronounced symptomatology of CAP according to NIH-CPSI questionnaire and moderately pronounced symptomatology according to IPSS with no intergroup differences (p > 0.05). Further dynamics of CAP symptoms according to NIH-CPSI pain and NIH-CPSI urination domains in the main group was characterized by progressive reduction of symptoms from 23 ± 6 points to 5 ± 2 points by the end of the course of SWT. The control group showed an increase in symptoms from 19 ± 7 to 25 ± 4 points at the start (week 2), with a tendency to decrease to 11 ± 3 points at week 12; there were significant intergroup differences (p < 0.05) throughout this time interval. It is encouraging that after the end of SWT in the control group there was a regression of symptomatology, comparable to the main observation group with stabilization of the effect up to 12 weeks (p > 0.05). The dynamics of LUTS according to IPSS was characterized by the growth of symptomatology in the control group against the background of SWT therapy from moderate to severe symptoms and subsequent reduction to mild symptoms. In the main group no similar effect on SWT therapy was observed (p < 0.05).
Conclusion. Thus, energy reduction during SWT by fractionation of the maximum pulse power to 1/3 of the standard one is accompanied by more pronounced symptomatology according to IPSS and NIH-CPSI questionnaires.
Introduction. In recent years, researchers have been paying special attention to the structure of the tumor microenvironment, which is assumed to be able to modulate the tumor behavior due to various paracrine factors and, thereby, act as a marker of the course and prognosis of prostate cancer (PCa). One of the components of the tumor microenvironment are cancer-associated fibroblasts (CAFs). Fibroblast activation protein (FAP) and plateletderived growth factor receptors α and β (PDGFR α and β) can be used as markers of CAFs.
Objective. To evaluate the association between the clinical and morphological features of PCa and CAFs markers, FAP and PDGFRα + β.
Materials & methods. The study used surgical material obtained from 34 patients with PCa. The age of the patients ranged from 52 to 77 years (mean age 64.1). The surgical material was stained with CAFs – FAP and PDGFRa + β markers. Subsequently, the relationship between these markers and the clinical and morphological features of PCa was analyzed using the RStudio software in the R programming language.
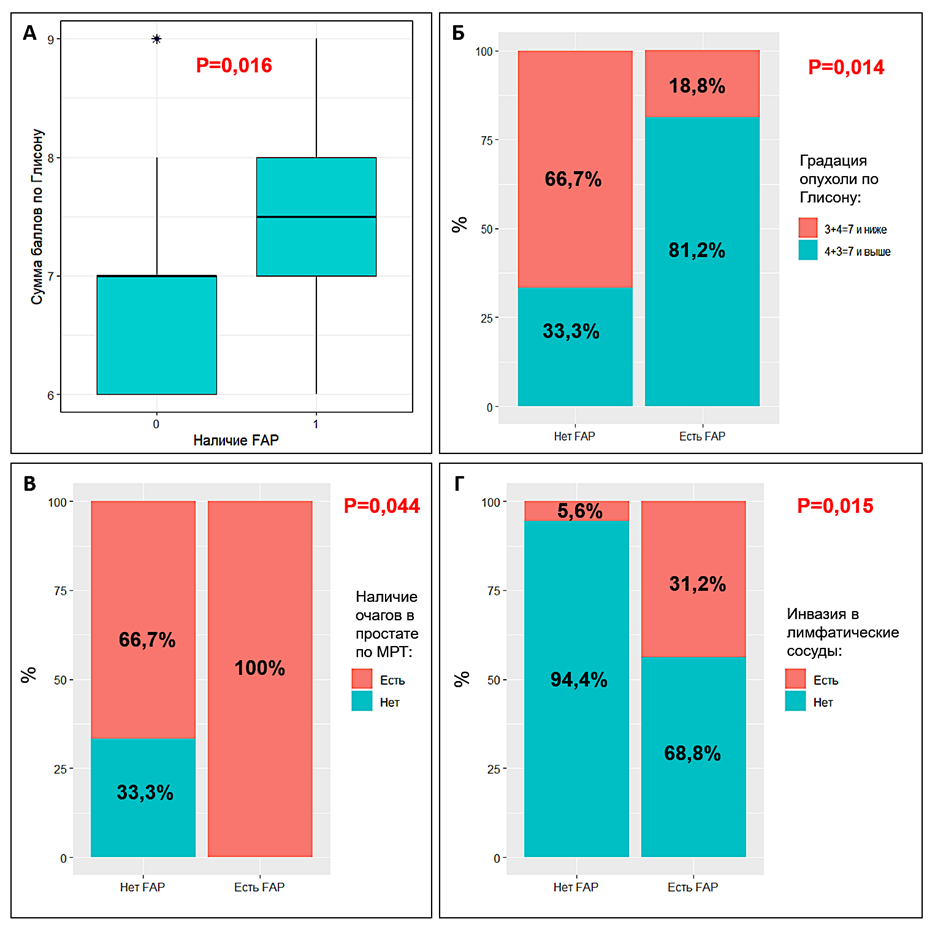
Results. A higher Gleason grade in the presence of FAP was noted: in 81.3% of cases, PCa was classified as Gleason 4 + 3 = 7 and higher, while in the absence of FAP, only 33.3% of tumors belonged to this category (p=0.014). In addition, patients with FAP were significantly more likely to have lymphatic invasion, which was detected in 43.8% of cases, while in the absence of FAP it was detected only in 5.6% (0.015). In the presence of FAP, patients were more likely to have a lesion of the prostate according to MRI, and lymph nodes were also more often affected (31.2% and 5.6%), however, this parameter had a borderline significance level (p = 0.078). With moderate/high PDGFRa + β expression, a higher Gleason grade was noted: in 80.0% of cases, PCa was classified as Gleason 4 + 3 = 7 and higher, while with no/ weak PDGFRa + β expression, only 36.8% of tumors belonged to this category (p = 0.030). In patients with moderate/ high PDGFRa + β expression, there was a more frequent probability of involvement of lymph nodes in the process (according to the MSKCC nomogram) and more likely to have lesions according to MRI at the borderline significance level of these parameters (p = 0.097 and p = 0.063, respectively).
Conclusion. The presence and severity of expression of stromal CAFs markers are associated with unfavorable clinical and morphological features of prostate cancer with a higher Gleason grade, more frequent lesions on MRI and the presence of invasion into the lymphatic vessels.
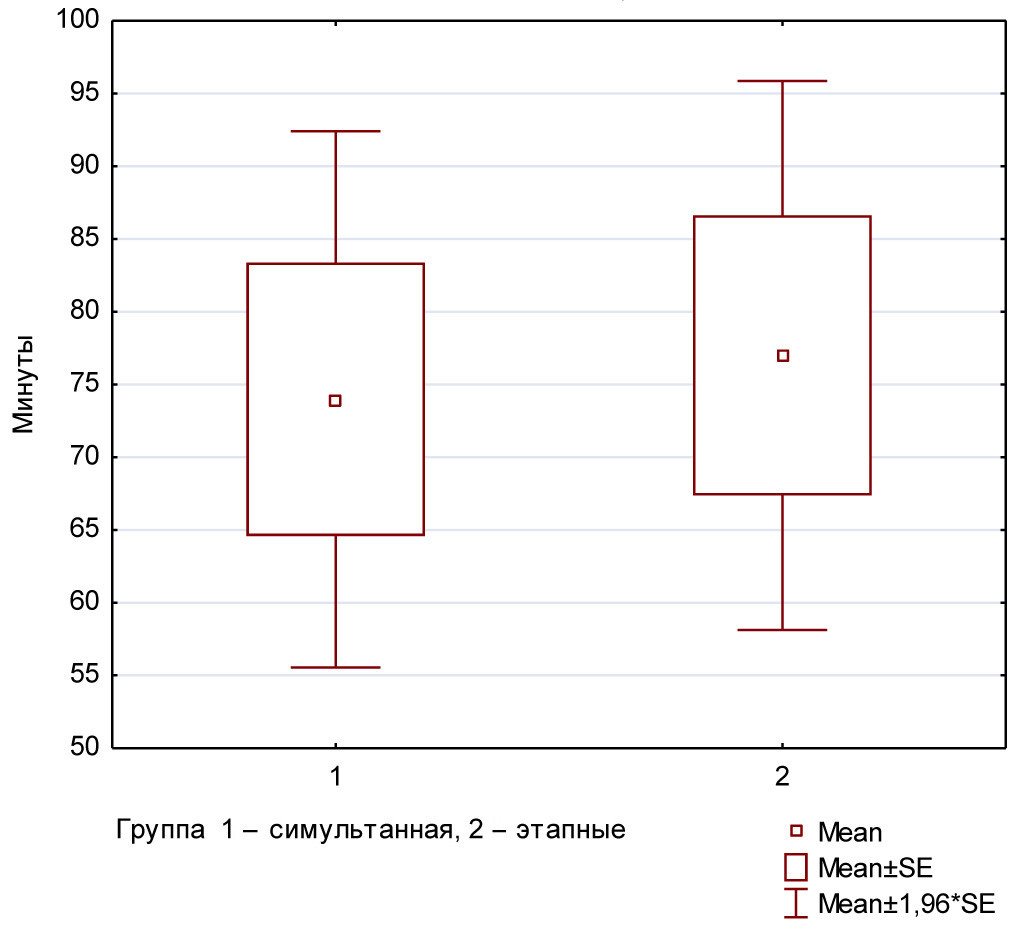
Introduction. Combined surgical pathology poses a dilemma between simultaneous and staged approaches. Simultaneous surgeries, performed during a single anesthetic session, reduce hospitalization time, lower anesthetic burden, however, increased operative volume and duration may elevate the risk of complications. The staged approach reduces the immediate burden on the patient but requires multiple hospitalizations, prolongs overall treatment and recovery time.
Objective. To compare clinical outcomes, length of hospitalization, postoperative complications and effectiveness of simultaneous versus staged urological surgeries within a structured enhanced recovery after surgery (ERAS) protocol.
Materials & methods. A prospective single-center randomized study evaluating the safety of simultaneous and staged urological surgeries included 78 patients with combined urological and surgical pathologies, randomized into two groups. Compliance with the ERAS protocol above 80% was a criterion for inclusion in both groups. Group 1 (n = 53) underwent simultaneous surgeries, where multiple procedures were performed during a single operative session. Group 2 (n = 25) received staged treatment, with surgical interventions separated in time. Perioperative parameters, complication rates according to the Clavien-Dindo classification, length of hospitalization, patient-reported outcomes including postoperative pain assessed by the visual analog scale (VAS), requirement for opioid analgesics, intraoperative blood loss, total duration of urinary drainage, and cumulative surgical access size were evaluated.
Results. Simultaneous surgeries demonstrated a significant reduction in overall hospitalization time (p < 0.01) and total operative time compared with staged interventions. No statistically significant differences in postoperative complication rates were observed between groups (p = 0.94).
Conclusion. Both simultaneous and staged urological surgeries are safe approaches for patients with combined pathology. Simultaneous interventions offer advantages including reduced hospitalization time without increasing the risk of postoperative complications.
REVIEWS ARTICLE
Introduction. The problem of assessing renal perfusion is especially relevant in purulent-destructive forms of pyelonephritis, since parenchymal infection is accompanied by foci of ischemia and necrosis. Visualization of perfusion allows you to identify such foci of reduced blood flow and diagnose complications in a timely manner. In recent years, new imaging techniques (e.g., CT perfusion, contrast-enhanced ultrasound, diffusion-weighted MRI) have emerged that have the potential to improve diagnostic accuracy.
Objective. To analyze modern methods for assessing renal perfusion in pyelonephritis and to formulate guidelines for clinical practice.
Material & methods. The review was carried out in accordance with the PRISMA rules. A systematic search of publications for the last 10 years (2013 – 2023) was carried out with the inclusion of key classical works for completeness of the analysis. The literature search was carried out in the international databases PubMed, Scopus, Web of Science, Cochrane Library, as well as in the Russian resources eLibrary and RSCI.
Outcomes. Contrast-enhanced CT (CECT) firmly occupies a leading position in a complicated course due to the combination of high sensitivity and informative value in relation to complications. The sensitivity of CT in the detection of parenchymal changes is about 80–90%, and the diagnostic accuracy is close to 90 – 95% in purulentdestructive forms. The ultrasound method, despite all its attractiveness (no harm, the possibility of performing it at the patient's bedside), is significantly inferior in sensitivity. Nevertheless, modern improvements in ultrasound technology radically increase the informative value of ultrasound. Some studies demonstrate results of CEUS comparable to CT (95 – 100% sensitivity). DMSA-scintigraphy is still the «gold standard» for scientific research on pyelonephritis in children. MRI has proven to be an excellent tool for diagnosing pyelonephritis in patients with contraindications to CT. PET/CT cannot be recommended for routine use in pyelonephritis, but the review shows its niche effectiveness in complex cases — when functional criteria for infection activity or a search for a latent focus are required.
Conclusion. Modern imaging methods make it possible to assess in detail the kidney perfusion in purulent pyelonephritis, significantly increasing the accuracy of diagnosis. The introduction of innovative technologies (CEUS, CT perfusion, functional MRI) opens new opportunities for early detection of complications and individualization of treatment, which ultimately improves the prognosis and contributes to the preservation of renal function in patients with this serious infection.
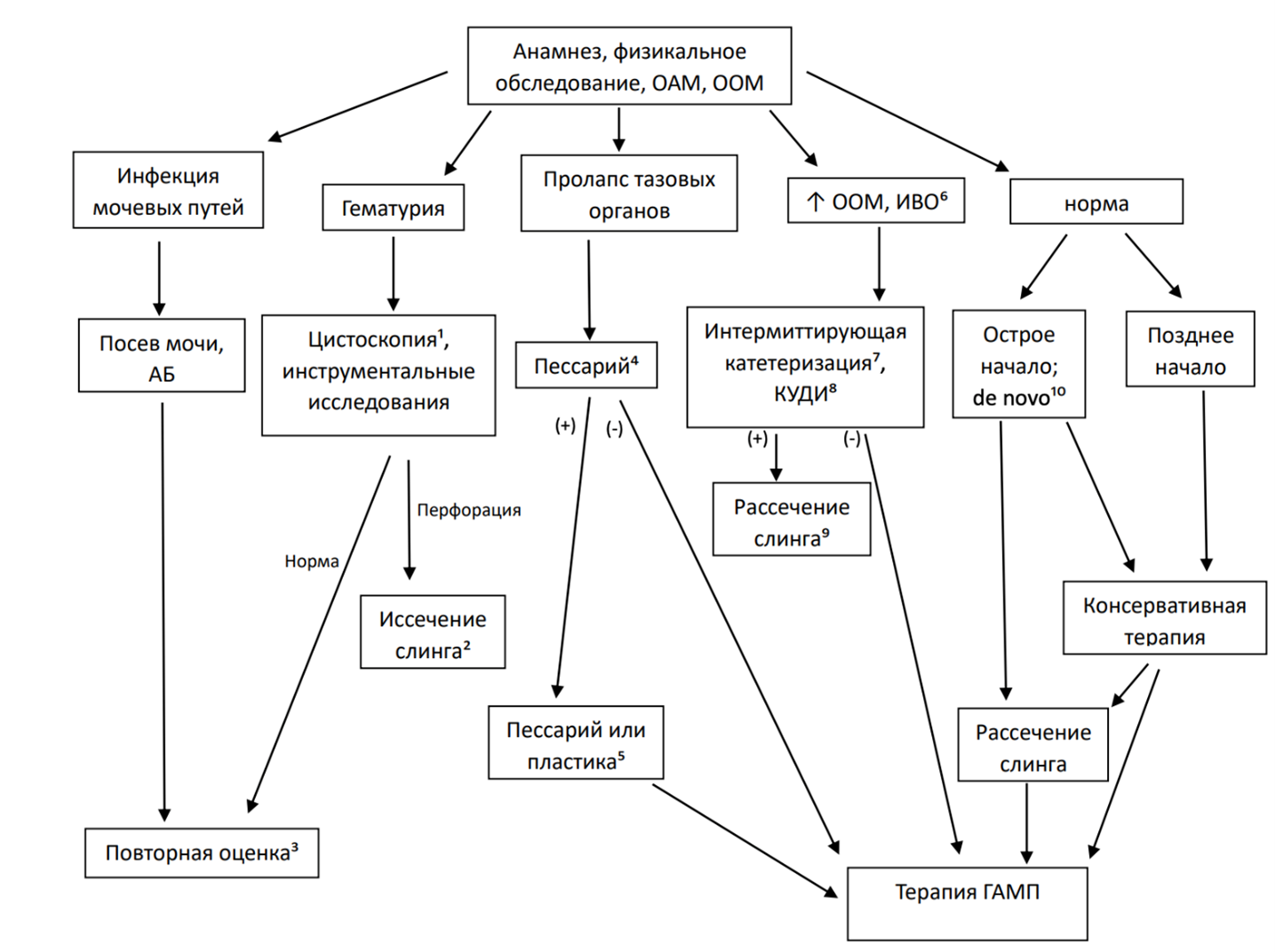
Introduction. Overactive bladder (OAB) de novo, while not considered a life-threatening condition, can be a significant issue for the patient. Moreover, urge urinary incontinence is more difficult to manage than stress urinary incontinence (SUI). Even in the absence of incontinence, this condition can significantly reduce the quality of life and satisfaction with the intervention.
Objective. To summarise the existing data on OAB de novo after midurethral loop implantation (MULI) and to analyse the risk factors for the development of this condition and the existing options for correction, with an assessment of the prospects for further clinical trials.
Materials & methods. The search for publications was performed on national and international abstract databases eLibrary.Ru, Pubmed, Cochrane Library. The following keywords were used for the search: ‘de novo hyperactivity’, ‘de novo urgency’, ‘de novo OAB’, ‘midurethral sling complications’, ‘hyperactivity after sling implantation’. A chronological limit of 20 years (2004-2024) was used. A total of 317 sources (publications from peer-reviewed periodicals) were retrieved. 234 publications were excluded after reading the abstract because they did not fit the assigned topic. For further analysis, 24 papers were selected from the remaining works that met the criteria of scientific reliability.
Results. According to the world literature, OAB de novo appears in 6.4% to 11.5% of patients who underwent MULI. However, there are studies where the above condition was observed in 41% of cases at 20-year follow-up. The underlying causes of involuntary bladder contractions may include various neurological diseases, inflammatory process, decreased activity of pelvic floor muscle tone inhibitors, increased neurotransmitter release, increased sensitivity to neurotransmitters, increased afferent innervation and infravesical obstruction. The mechanism for the development of OAB de novo remains an ongoing challenge.
Conclusion. Any surgical intervention to correct SUI may lead to adverse effects, in particular OAB de novo. Information on the prevalence of this condition, as well as on approaches to its treatment, varies from study to study. There is a high percentage of underestimation of urgency symptoms at the preoperative stage. Therefore, a more detailed history should be taken and targeted investigations should be carried out at the initial consultation. OAB de novo following MULI significantly reduces patients' quality of life and satisfaction with the treatment.
EXCHANGE OF PRACTICAL EXPERIENCE
Introduction. Benign prostatic hyperplasia (BPH) is the most common cause of bladder outlet obstruction in men over 50 years old who have lower urinary tract symptoms.
Objective. To investigate the impact of intravesical prostate protrusion (IPP) during sonography concerning the response to medical treatment in patients with BPH.
Materials & methods. This study is a descriptive-analytical quasi-experimental. The individuals (80 patients) were divided into two groups based on the presence or absence of IPP as seen in ultrasound. Before and after one month of treatment with the alpha-blocker, PVR and IPSS were measured in the patients, and the improvement trends in the two groups were compared.
Results. The mean age of patients in both groups was 66.08 ± 10.8 years. After treatment with alpha-blockers, the mean PVR in IPP-patients was 6.82 ± 5.6 ml, and in no-IPP-patients it was 25.37 ± 15.57 ml (P > 0.001). After treatment with alpha-blockers, the mean score in IPP-patients was 6.78 ± 9.52, and in no-IPP-patients it was 12.55± 6.99 (P = 0.388).
Conclusion. The results indicate that the effect of the alpha-blocker medication on patients with IPP was greater than on those without IPP, highlighting the positive impact of using alpha-blockers in patients with BPH who have IPP.

Introduction. Organ-preserving treatment for localized renal cell carcinoma requires the use of renal warm ischemia (RWI). Establishing access to the renal vessels is a surgical procedure associated with a high risk of bleeding. However, RWI, once blood flow is restored, can cause ischemia-reperfusion injury to the renal parenchyma. An alternative to standard RWI is temporary balloon occlusion (TBO) of the renal artery using a dual-lumen Fogarty catheter. TBO offers comparable advantages in ensuring intraoperative hemostasis and a comparable safety profile, particularly in repeat interventions for neoplasms in the ipsilateral kidney.
Objective. To evaluate the outcomes of laparoscopic partial nephrectomy (LPN) for neoplasms using RWI of the renal artery compared to LRN under TBO.
Materials and Methods. Between September 2022 and November 2024, seven patients with localized RCC (tumor size £ 4.8 cm) underwent treatment. Analysis focused on surgery duration, procedural steps, intraoperative blood loss, oncological radicality as per histopathological examination, intraand postoperative complications, and length of hospital stay.
Results. The following advantages were found for LPN under TBO (n = 7) compared to LRN under RWI (n = 78, based on a previous study): 1) comparable surgical time; 2) identical hospital stay; 3) threefold reduced intraoperative blood loss; 4) absence of infectious and inflammatory complications. The study identified additional advantages of LRN under TBO: no risk of damage to the structural elements of the renal vessels during dissection, especially in patients with repeated interventions on the same side; radical intervention; and the ability to reduce the degree of ischemia-reperfusion injury to the remaining renal parenchyma due to the possibility of selective occlusion of renal artery branches.
Conclusion. TBO of the renal artery branches feeding the tumour, along with minimally invasive organ-preserving treatment for RCC, allows for improved functional outcomes. This is achieved by mitigating the risk of damage to the renal vessels, reducing intraoperative blood loss, and eliminating the need for RWI, which is associated with alteration of the preserved renal tissue.
Introduction. The combination of urolithiasis with other diseases and/or malformations, especially abnormally developed kidneys and urinary tract, presents a certain complexity for the diagnosis of the underlying disease and its complications, as well as for the initial, repeated and subsequent treatment of patients. One of the abnormalities in the development of the kidneys is the horseshoe shape. It is the most common variant of fusion and, according to domestic and foreign literature, occurs in approximately 0.25% (1:500 – 1:400) of the population.
Objective. To determine the most optimal approach when performing percutaneous nephrolithotripsy on horseshoe kidneys, analyzing intraand postoperative complications, the number and size of residual stones.
Materials & methods. In the period from November 2020 to March 2024, 12 patients — 8 (66.7%) men and 4 (33.3%) women) with horseshoe kidneys were treated. The size of the stones ranged from 2.0 to 2.5 cm (2.26 ± 0.16 cm), the density of the stones averaged 1083.3 ± 54.7 HU (from 1020 to 1200 HU). Surgical treatment of urolithiasis in patients included in the study was carried out using standard percutaneous nephrolithotripsy (PNL) adjusted for renal adhesion and atypical location. All patients underwent spiral CT with intravenous contrast, which made it possible to clarify and assess the size and density of the stone; stereometric location, morphological and functional state of the horseshoe kidney, its skeletotopia, syntopy and holotopia, as well as blood supply.
Results. The technique of access through the upper calyx in the treatment of urolithiasis in patients with horseshoe kidney demonstrates high safety and effectiveness. The absence of bleeding and the relatively low incidence of residual stones indicate the reliability of this approach.
Conclusions. The results of the study confirm a significant superiority of access through the upper calyx in the surgical treatment of urolithiasis in patients with a horseshoe kidney. This method has shown high efficiency and safety minimizing the risk of complications and providing sustainable clinical results.








































