




Contents
Scroll to:
https://doi.org/10.21886/2308-6424-2021-9-1-113-117
Scroll to:
A case of the ureteral tumour endoscopic treatment is presented in a patient with primary multiple malignancies. In the case of polyneoplasia, there are usually two or more neoplasms of different localizations, including the organs of the urinary system. The kidney and prostate tumours are diagnosed more often, but in rare cases, ureter neoplasms. It is especially important to perform organ-sparing surgeries when diagnosing ureter neoplasms. In addition, chronic kidney disease after radical nephroureterectomy can be a relative contraindication to further chemoradiation therapy in polyneoplasias. In this patient, along with the breast and vulva neoplasms, a solitary tumour of the right ureter's lower third was detected, which was successfully removed endoscopically. The chosen method of minimally invasive treatment allowed to preserve a normal functioning kidney, to avoid the development of chronic kidney disease in the patient, who was later scheduled for chemotherapy.
Guliev B.G., Komyakov B.K., Avazkhanov Zh.P. Endoscopic laser resection of a ureteral tumour in primary multiple malignant neoplasms. Urology Herald. 2021;9(1):113-117. (In Russ.) https://doi.org/10.21886/2308-6424-2021-9-1-113-117
Diagnostics and therapy of primary multiple malignant neoplasms (PMMNs) remain a complicated issue in modern oncology. The dynamics of the rate of patients with PMMNs increased in Russia during the past decade. In 2011, there were 24,774 cases of PMMNs revealed, and in 2018 ― 54,873, which was 4.7% and 8.8%, respectively, of all primary revealed neoplasms [1]. The most frequent PMMNs are observed in the gastrointestinal tract and female reproductive organs [2][3]. The occurrence rate of polyneoplasia in urology varies from 4.7% to 16.8% [4][5][6]. In cases with PMMNs, simultaneous surgeries can be performed that provide quick removal of all malignant neoplasms. Still, there are difficulties in the algorithm of manipulations in the case of a combination of urinary system tumor and oncopathology of other localizations. This is associated with the difference in the tactics of these pathologies treatment. Isolated PMMNs are a complicated task for a complex surgical and chemotherapeutic treatment. This can be explained by the differences in the biology of malignant tumors of different organs, which determine the differences in the volume of surgical treatment and the schemes of chemotherapy. The most frequent are prostate and kidney tumors, the rarest localizations of tumors are ureters among PMMNs oncourological diseases. [1][4][5]. Neoplasms in the upper urinary tract (UUT) are primarily revealed by excretory or CT-urograms as defects of filling. Urethroscopy and biopsy are performed for their histological verification and grade identification [7][8]. The choice of the treatment method for these patients should be made in favor of organ-spearing techniques. Among them, the most low-invasive method is considered to be the removal of the ureteral tumor [8][9][10][11]. In the case of technical impossibility of this type of intervention and the localization of the tumor in the ureter’s lower third, the resection of this area can be made by the method of ureterocystoneostomy according to Boari or intestinal segment plasty. The present article describes a case of endoscopic removal of a ureteral tumor in a patient with PMMNs.
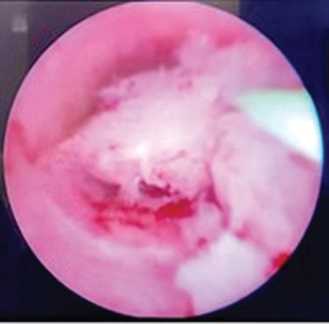
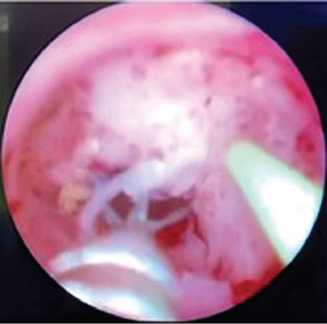
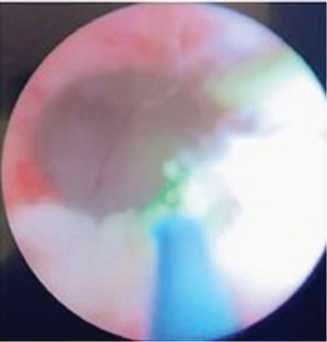
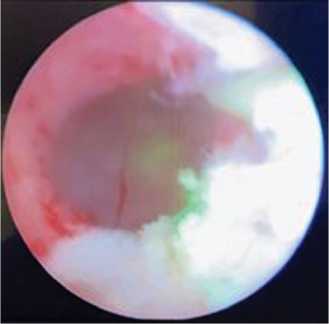
Patient Т. aged 68 years old was hospitalized to the clinics with PMMNs. The anamnesis said that in April 2020, a biopsy of the neoplasm in the left breast was taken. Histological study revealed non-specific invasive cancer (T1N1M0). Anastrozole chemotherapy was indicated. In July 2020, a vulva tumor was diagnosed. Extended vulvectomy with the plasty of the formed defect with local tissues was performed. Histological findings showed keratinizing squamous cell carcinoma of the vulva (G2, 1.5 cm long, depth of invasion 6mm) without the signs of lymphovascular invasion. In one out of 13 inguinofemoral lymph nodes, metastasis was revealed. Further, the patient was followed up by the local oncologist. Control abdominal and pelvic MRI revealed a neoplasm in the ureter’s lower third. The tumor was 1.5 cm in diameter and had an expansion of UUT on the right. Cytological study of the urine did not show signs of atypia. The patient was diagnosed with a tumor of the right ureter’s lower third and right-side hydroureteronephrosis. Cystoscopy was performed on 14.01.2021. The bladder was without peculiarities, ureteral orifices were located typically and symmetrically. The surgeons introduced a rigid ureteroscope 9.5 Сh. Exophytic soft villous neoplasm was visualized 5 cm higher than the ureter orifice that closed the ureter lumen (Fig. 1). Examination with a rigid ureteroscope did not reveal other tumors. Dormia’s loop was used to perform a biopsy and remove the main exophytic part of the tumor (Fig. 2). Further, the tumor’s base laser incision and bleeding vessel coagulation were performed (Fig. 3, 4). The guidewire was used to install a stent 7 Ch.
Intra and postoperative complications were not registered. The patient was discharged for further outpatient treatment by day 2. Histological findings showed high-grade intraepithelial urothelial carcinoma, pTa N0M0.
The patient was followed-up by the authors and continued the treatment for the breast and vulva tumors. The ultrasonic examination showed that the right renal cavitary system was not expanded. The renal end of the stent was visualized in the renal pelvis. The authors plan to perform a repeated ureteroscopy with biopsy of the ureteral wall in the area of the removed tumor and laser ablation after the end of the treatment for the other two oncological diseases
The treatment of patients with PMMNs has certain complications. In their practice, urologists face patients with urinary system tumors combined with tumors of other localizations. The volume of urological surgery can depend on the patient’s age, general condition, characteristics of the diagnosed neoplasms, including oncourological. The treatment tactics for urothelial tumors in the upper urinary tract depend on the localization and progress of the oncological process and functional condition of the affected and the contralateral kidney [8][10]. If a tumor is localized in the pyelocalyceal system with seeding of tumor cells downwards along the ureter and normal contralateral kidney, an absolute indication is radical nephroureterectomy with the resection of the bladder. In the cases of single neoplasms in the UUT, especially, in the only or only functioning kidney, organ-sparing surgery can be performed [8]. As for the pathway of the UUT urogenital cancer metastasizing, if it is localized in the ureter’s lower third, resection of this part of the ureter is performed along with Boari’s ureterocystoneostomy or ileoureteroplasty. The implementation of endoscopic and laser technologies increased the share of organ-sparing surgeries in patients with UUT tumors. Technical possibilities of modern rigid ureteroscopes allow the surgeons to perform resections of not only the ureter and renal pelvis but also all groups of calices. NBA method improves the visualization and diagnostics of minor neoplasms [9]. Further, flexible forceps can be used to perform the biopsy. Then, laser incision of the tumor base with bleeding vessels coagulation can be carried out. Considering the low invasiveness of endoscopic interventions, they can be performed on patients with single neoplasms for elective indications.
Organ-sparing endoscopic interventions for UUT tumors are especially relevant in patients with PMMNs. In such patients, oncologic diseases of other organs may require vast surgical treatment or polychemotherapy. The removal of a normally functioning kidney leads to the development of chronic kidney disease, which is a relative contraindication for chemoradiation therapy. Thus, for such patients, kidney-spearing surgery is feasible. This surgery was performed on the patient who was scheduled for the continuation of the polychemotherapy. The authors plan the repeated ureteroscopy for the evaluation of the area of surgery, biopsy, and possible laser ablation after the required therapy indicated by other specialists.
In rare cases, ureter tumors are revealed in patients with polyneoplasia. Low-invasive organ-sparing techniques allow the surgeons to preserve the functioning of the kidney and avoid the development of chronic kidney disease. Thus, the patient could have chemoradiation therapy as a part of further therapy.
1. Kaprin A.D., Stalinskiy V.V., Petrova G.V., eds. Malignancies in Russia in 2018 (morbidity and mortality). Moscow: P.A. Gertsen MNIOI; 2019. (In Russ.). ISBN 978-5-85502-243-8
2. Payanidi Y.G., Zhordania K.I., Pauker V., Selchuk V.Y., Kazub-skaya T.P. Polyineoplasia of female reproductive system organs and heredity. Obstetrics and gynecology. 2016;9:68-72. (In Russ.). DOI: 10.18565/aig.2016.9.68-72
3. Vasilyev N.V., Markovich V.A., Frolova I.G., Ermolenko R.V., Maltseva A.A., Kovalev О.Е, Lyutikova P.G. Polyneoplasia associated with gastrointestinal stromal tumor: literature review and case report. Siberian journal of oncology. 2020;19(2):140-146. (In Russ.). DOI: 10.21294/1814-4861-2020-19-2-140-146
4. Kinoshita Y, Singh A, Rovito PM Jr, Wang CY, Haas GP. Double primary cancers of the prostate and bladder: a literature review. Clin Prostate Cancer. 2004;3(2):83-6. DOI: 10.3816/cgc.2004.n.016
5. Leonov O.V., Dolgikh V.T., Kopyltsov E.I., Alekseev B.Y. Primary-multiple malignant neoplasms involving the urinary tract. Cancer Urology. 2010;2:56-61. (In Russ.). DOI: 10.17650/1726-9776-2010-6-2-56-60
6. Dong C, Hemminki K. Second primary neoplasms in 633,964 cancer patients in Sweden. Int J Cancer. 2011;93(2):155-161. DOI: 10.1002/ijc.1317
7. Martov A.G., Solomatnikov I.A., Baykov N.A., Andronov A.S., Khalmurzaev O.A. Narrowed spectrum diagnostics and computer chromoendoscopy in the diagnosis of epithelial neoplasms of the lower and upper urinary tract. Urology. 2015;(5):55-59. (In Russ.). eLIBRARY ID: 24881912
8. Roupret M., Babjuk M., Burger M., Capoun O., Cohen D. et al. Comperat EM, Cowan NC, Dominguez-Escrig JL, Gontero P, Mostafid AH, Palou J, Peyronnet B, Seisen T, Soukup V, Sylvester RJ, van Rhijn BWG, Zigeuner R, Shariat SF. European association of urology guidelines on upper urinary tract urothelial carcinoma: 2020 Update. Eur Urol. 2021;79(1):62-79. DOI: 10.1016/j.eururo.2020.05.042
9. Komyakov B.K., Guliyev B.G., Makovskaya A.I., Kim V.E., Idrisov S.N. Percutaneous endoscopic electrosection of pelvic tumors. Cancer Urology. 2011;1:85-89. (In Russ.). DOI: 10.17650/1726-9776-2011-7-1-85-89
10. Rai BP, Shelley M, Coles B, Somani B, Nabi G. Surgical management for upper urinary tract transitional cell carcinoma (UUT-TCC): a systematic review. BJU Int. 2012;110(10):1426-1435. DOI: 10.1111/j.1464-410X.2012.11341.x
11. Martov A.G., Ergakov N.G., Muzhetskaya R.G., Biktimirov R.G., Andronov A.S., Shoaydarov M.A. Endoscopic removal of a papillary tumor of the ureter in a patient with polyneoplasia. Experimental and clinical urology. 2020;13(5):42-45. (In Russ.). DOI: 10.29188/2222-8543-2020-13-5-42-45
Bakhman G. Guliev — M.D., Dr. Sc. (M), Full Prof.; Prof., Dept. of Urology, Mechnikov North-West State Medical University; Head, Urology Centre with Robot-assisted Surgery.
191015, St. Petersburg, 41 Kirochnaya st.; 191014, St. Petersburg, 56 Liteiny ave. ; tel.: +7 (921) 945-34-80
BorisK. Komyakov — M.D., Dr. Sc. (M), Full Prof.; Head, Dept. of Urology.
191015, St. Petersburg, 41 Kirochnaya st.
Zhaloliddin P. Avazkhanov — M.D.; Urologist, Urology Centre with Robot-assisted Surgery, St. Petersburg Mariinsky Hospital; Post-graduate student, Dept. of Urology.
191015, St. Petersburg, 41 Kirochnaya st.; 191014, St. Petersburg, 56 Liteiny ave.
Guliev B.G., Komyakov B.K., Avazkhanov Zh.P. Endoscopic laser resection of a ureteral tumour in primary multiple malignant neoplasms. Urology Herald. 2021;9(1):113-117. (In Russ.) https://doi.org/10.21886/2308-6424-2021-9-1-113-117

Editor-in-Chief
 Vladimir P. Glukhov
Vladimir P. Glukhov
29 Nakhichevanskiy Ln., Rostov-on-Don, 344022, Russian Federation, Rostov State Medical University, Department of Urology and Pediatric Urology
Phone: +7 (863) 201-44-48
e-mail: urovest@mail.ru






































