


ORIGINAL ARTICLES
Introduction. Urolithiasis ranks among the most common and socially significant urological conditions. Male sex and advancing age are well‑recognized risk factors for stone disease. In the general population, the likelihood of urolithiasis rises with age. At the same time, men and women differ not only in the prevalence of urolithiasis but also in the pattern of sex‑specific risk factors.
Objective. To assess the age-gender characteristics of the urolithiasis.
Materials & methods. The present study included 23464 patients hospitalized in the Urology division of Savelieva Moscow City Clinical Hospital No. 31 from 2019 to 2024. The study group of patients consisted of patients with an established diagnosis of urolithiasis, while all other patients without urolithiasis formed the control group.
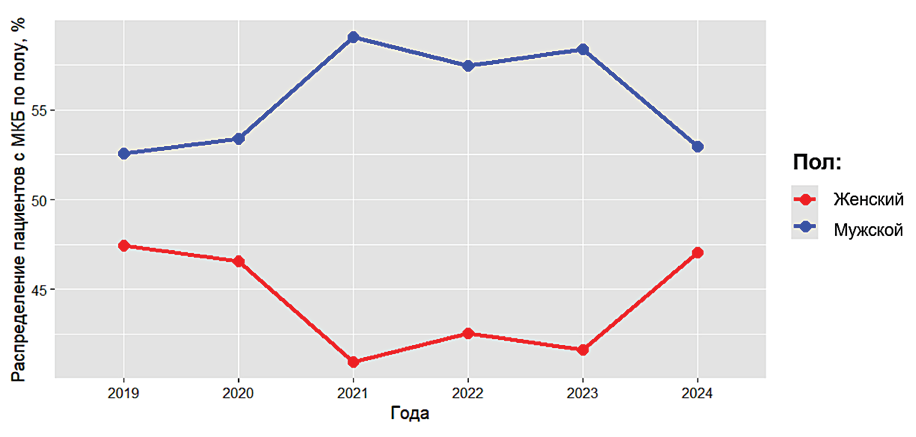
Results. Urolithiasis was identified in 38.2% of respondents (8,972 patients). Among patients with urolithiasis, 55.9% were men (mean age 50.1 years) and 44.1% were women (mean age 54.5 years). The prevalence of urolithiasis in men increases steadily with age and reaches a plateau between 30–34 and 45–49 years. The highest odds of urolithiasis are observed in the 35–39-year age group: in these patients, the odds are 4.3-fold higher than in men aged 18–24 years (OR 4.326; 95% CI 3.433–5.449; p < 0.001), corresponding to a 68.8% probability of urolithiasis. Thereafter, the odds of urolithiasis gradually decrease. In women, the prevalence of urolithiasis also increases with age, peaking at 60–64 years. Thus, in women aged 60–64 years, the odds of urolithiasis are 3.4-fold higher than in those aged 18–24 years (OR 1.553; 95% CI 1.242–1.943; p < 0.001), corresponding to a 53.7% probability of urolithiasis. In patients aged 65 years and older, the odds of urolithiasis remain consistently high.
Conclusion. Advancing age in men is associated with a lower probability of urolithiasis, whereas advancing age in women is associated with a higher probability of urolithiasis. These patterns may reflect age‑related changes in sex hormone levels, with androgens regarded as promoters of stone formation and estrogens as inhibitors of stone formation.
Introduction. Chronic kidney disease (CKD) is a major medical and public health problem and is accompanied by a broad spectrum of complications, including erectile dysfunction (ED) and disorders of reproductive health, which substantially impair quality of life in affected men and may be further exacerbated by renal replacement therapy (RRT).
Objective. To evaluate the impact of hemodialysis as a form of RRT on erectile function and reproductive health in men with CKD.
Materials& methods. A prospective study was conducted in 201 male patients with CKD receiving scheduled hemodialysis (mean age 35.2 ± 1.9 years). Erectile function was assessed using the International Index of Erectile Function (IIEF‑5); penile hemodynamics were evaluated by duplex Doppler ultrasonography of the penile arteries; hormonal status was characterized by serum testosterone, luteinizing hormone, and follicle‑stimulating hormone levels; and reproductive function was evaluated by semen analysis and testicular volume at three time points: baseline (severe azotemia) and 12 months after initiation of RRT. ED therapy included phosphodiesterase type‑5 inhibitors (5 mg once daily for 3 months, then 20 mg on demand), targeted pelvic‑floor exercises, vacuum therapy, and physiotherapy.
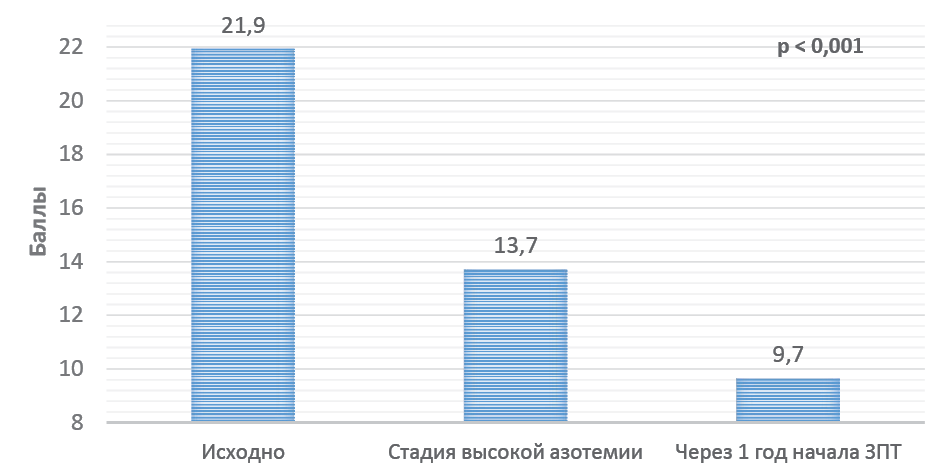
Results. ED progressed over time, with mean IIEF‑5 scores declining from 21.9 to 9.7 points (p < 0.001), and the proportions of patients with mild‑to‑moderate, moderate, and severe ED rising to 20.4%, 65.7%, and 13.9%, respectively. Mean peak systolic velocity in the right cavernosal artery decreased from 6.5 ± 0.1 to 4.8 ± 0.1 cm/s (p < 0.001); serum testosterone from 5.1 ± 0.2 to 4.0 ± 0.2 ng/ml (p < 0.001); luteinizing hormone from 8.9 ± 0.1 to 6.9 ± 0.1 (p < 0.001); follicle‑stimulating hormone from 6.3 ± 0.1 to 5.0 ± 0.1 (p < 0.001); and the prevalence of normozoospermia from 59.2% to 50.7% (p < 0.001), with a concomitant increase in pathological spermatogenesis (asthenozoospermia, oligozoospermia, oligo-astheno-teratozoospermia) to 14.0% (p < 0.001).
Conclusions. CKD and hemodialysis are associated with multifactorial impairments of erectile and reproductive function driven by vascular, hormonal, and structural alterations.
Introduction. Interstitial cystitis/bladder pain syndrome (IC/BPS), being a chronic non-infectious disease, still has an unclear etiology and numerous pathophysiological theories of development. This determines the need for preclinical experimental studies on animals. The most identical model of human IC/BPS is cyclophosphamide-induced cystitis in rodents.
Objective. To study the effects of the pharmacological activity of Neovasculgen® сompared to Botox® using model of cyclophosphamide-induced IC/BPS in rats.
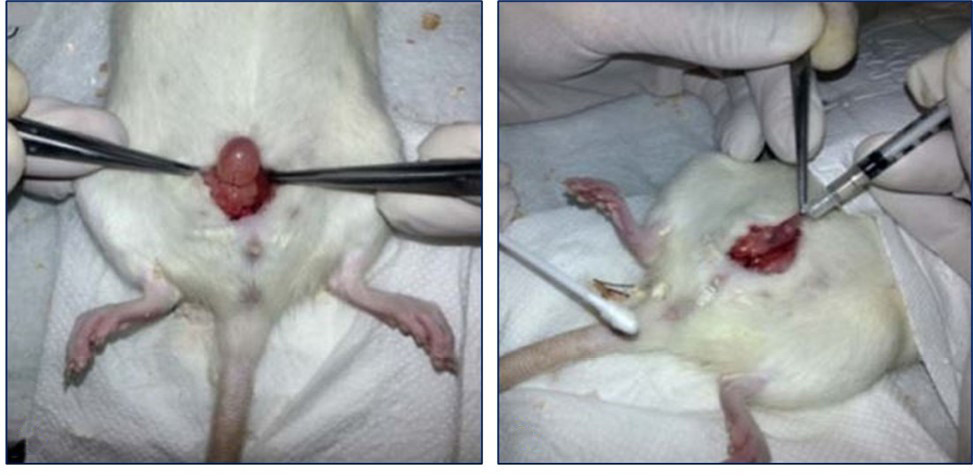
Materials & methods. The study was performed on 90 female Wistar rats. IC/BPS was induced by Endoxan®. Neovasculgen® and Botox® were used as intradetrusor therapeutic agents. Efficiency was assessed by comparative analysis of urodynamic patterns and morphologically. The data obtained were processed by parametric and nonparametric methods of statistical analysis.
Results. Cyclophosphamide-induced IC/BPS developed in all animals. Both drugs statistically significantly improved the studied urodynamic parameters, the clinical efficacy of Neovasculgen® was comparable to Botox®. Morphological assessment showed that the administration of the studied drugs was accompanied by a decrease in tissue edema, less pronounced hemorrhages and focal lymphohistiocytic infiltration, as well as destructive changes in the bladder mucosa. At the same time, the intensity of pathological tissue processes against the background of the administration of Neovasculgen® was the lowest.
Conclusions. The cyclophosphamide-induced IC/BPS model is considered the most adequate human IC/BPS. The experiment is extremely important for studying the effectiveness of a new drug, which is intradetrusor Neovasculgen®. The drug has shown its effectiveness in reducing the frequency of urination and intravesical pressure. Intradetrusor administration reduces the severity of the inflammatory reaction of bladder tissue.
Introduction. Deep endometriosis (DE) represents the most severe form of the disease, in which not only the reproductive system but also adjacent organs are affected, leading to serious complications. The urinary tract is the second most commonly involved system in deep endometriosis.
Objective. To study the clinical and anamnestic features of the course of deep infiltrating endometriosis with involvement of the bladder.
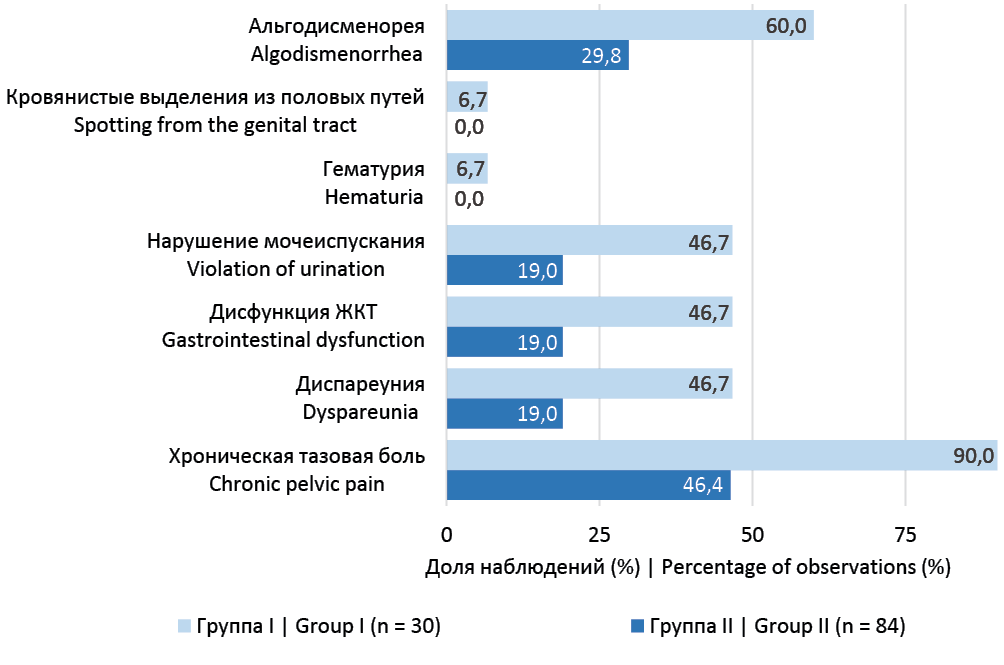
Materials & methods. A retrospective analysis was conducted of 114 patients undergoing surgical treatment for deep infiltrative endometriosis from three institutions placed in Ekaterinburg from 2021 to 2024. Patients were divided into two groups according to the presence (group 1, n = 30) or absence (group 2, n = 84) of involvement of the urinary bladder or the vesicouterine pouch.
Results. Symptom intensity prompting women to seek medical attention typically emerges from around 30 years of age. The interval between the first consultation for endometriosis-related complaints and the date of surgery was 11.6 [7.0; 37.1] months in group 1 and 13.1 [4.7; 31.5] months in group 2 (p = 0.450). The most frequent presenting symptom was chronic pelvic pain, observed in 66/114 (60.0%) patients overall: 27/30 (90.0%) in group 1 and 39/84 (46.4%) in group 2 (p = <0.001). LUTS were significantly more common in women with detrusor involvement in the endometriotic infiltrate: 14/30 (46.7%) in group 1 vs16/84 (19.0%) in group 2 (p = <0.001). Urinary symptoms usually manifested 1–2 days before the onset of menstruation or on the first day of bleeding. In all cases, the endometriotic infiltrate involved the posterior wall of the bladder body. Laparoscopic partial cystectomy was performed in 17/30 (50.0%) patients.
Conclusions. Women with deep endometriosis involving the bladder generally experience a more severe disease course. Bladder involvement in deep endometriosis is typically seen in the context of recurrent disease. When bladder endometriosis is suspected, careful evaluation of the posterior wall of the bladder body is particularly warranted.
Introduction. Renal biopsy is a common procedure in patients with nephrological and onco-urological diseases. Histopathological examination of renal tissue is performed to clarify the diagnosis and stage of the pathological process, to guide treatment strategy, and to assess prognosis. Thus, renal biopsy has become an integral component of current clinical practice for a wide range of renal disorders.
Objective. To assess the safety and diagnostic effectiveness of renal biopsy in various pathological conditions and to analyze the spectrum, patterns, and risk factors of post‑biopsy complications.
Materials & methods. A retrospective analysis was performed of patients who underwent percutaneous kidney biopsy between January 2018 and September 2023. The study included 1,201 patients aged 18 to 84 years. Biopsy for a renal tumor was performed in 24 (2.1%) patients, and 1,177 (97.9%) patients underwent biopsy for nephrological indications (evaluation of renal disease or characterization of renal dysfunction, including renal failure). Post‑biopsy events were graded according to the Clavien–Dindo classification. A complication was considered severe if it required interventions such as blood transfusion or radiological or surgical procedures.
Results. Of the 1,201 patients, 625 (52%) were men (mean age 57 ± 15 years) and 576 (48%) were women (mean age 55 ± 17 years). The diagnostic yield did not differ between patients from whom two or more cores were obtained; its value increased from 83% to 91% and was significantly higher than in cases with only one core (46.4%, p = 0.002). Post‑biopsy complications occurred in 122 patients. Major complications were observed in 15 (1.2%) patients; 1 patient (0.08%) required urgent nephrectomy, and 9 (0.7%) underwent angiography with renal artery embolization. No procedure‑related deaths were recorded. In most cases (n = 112; 91.8%), clinically relevant changes were detected within the first 6 hours after biopsy. The highest complication rates were observed in women, in younger patients, in those with higher azotemia, and in patients with elevated INR and reduced prothrombin index values; complications were also more frequent in patients with arterial hypertension. Blood transfusion corresponded to Clavien–Dindo grade III–IV complications. The incidence of complications in the postoperative period was higher in patients who required four needle passes (p = 0.044).
Conclusion. Kidney biopsy is a minimally invasive and generally safe procedure. Obtaining two cores of renal tissue is sufficient to ensure adequate diagnostic yield while minimizing the risk of complications. Careful pre‑procedural assessment and correction of modifiable risk factors (such as arterial hypertension and coagulopathy), together with close monitoring for at least six hours after the procedure, helps keep the risk of post‑biopsy complications to a minimum.
Introduction. Prostate biopsy remains the gold standard for the diagnosis of prostate cancer. In contemporary practice, increasing preference is given to fusion biopsy, which is more reliable and informative than conventional ultrasound‑guided systematic biopsy. Fusion prostate biopsy can be performed via transrectal or transperineal access, and the superiority of one approach over the other is still under investigation.
Objective. To assess and compare the diagnostic performance of transrectal versus transperineal fusion prostate biopsy for the detection of prostate cancer.
Materials & methods. A comparative study was conducted between October 2024 and January 2025 at St. Luke’s Clinical Hospital, Saint Petersburg. A total of 162 men with suspected prostate cancer were enrolled. Group 1 comprised 115 patients who underwent transrectal fusion prostate biopsy. Group 2 included 47 patients who underwent transperineal fusion prostate biopsy using a stabilized technique with a stepper and stabilizer.
Results. In the transrectal fusion biopsy group, prostate cancer was identified in 54 cases (46.95%) on targeted cores and in 81 cases (70.4%) on standard systematic cores. Systematic cores alone detected cancer in 44 patients (38.26%), whereas targeted cores alone did so in 5 patients (4.34%); in an additional 6 patients (5.22%), targeted cores upgraded the Gleason score. Omitting systematic sampling in transrectal fusion biopsy would have reduced overall cancer detection by 38.26%, including omission of clinically significant (aggressive) disease in 9.57% of cases. In the transperineal fusion biopsy group, cancer was detected in 31 patients (65.96%) on targeted cores and in 25 patients (53.19%) on systematic cores. Targeted cores alone identified cancer in 9 cases (19.15%), whereas systematic cores contributed only 3 additional cases (6.38%), all ISUP grade group 1. Targeted sampling led to Gleason score upgrading in 4 patients (8.51%).
Conclusions. For the transperineal fusion technique, omitting systematic biopsies may reduce the number of cores without materially compromising diagnostic accuracy. In contrast, for transrectal fusion biopsy, systematic sampling remains crucial, particularly for detecting aggressive cancers and improving overall diagnostic yield. These approach‑specific differences warrant further investigation to refine diagnostic pathways for prostate cancer.
Introduction. Renal trauma accounts for 2–10% of all injuries to the urinary system. The optimal management strategy for renal trauma with collecting system rupture remains controversial. Over the past decade, accumulating evidence has demonstrated the high efficacy of non‑operative management (NOM) in this setting.
Objective. To determine the optimal management approach for blunt renal trauma with collecting system rupture.
Materials & methods. From 1998 to 2023, 43 patients with blunt renal trauma complicated by collecting system rupture were treated at the Dzhanelidze Research Institute of Emergency Medicine. The severity of renal injury was graded according to the American Association for the Surgery of Trauma (AAST) classification. The severity of traumatic shock was assessed using the Y.N. Tsibin scoring system. Patients were divided into two groups. Management strategies for blunt renal trauma with collecting system rupture included both conservative and surgical approaches.
Results. The median age of the patients was 43 years (interquartile range 35 – 55), and the male-to-female ratio was 32:11. In the prospective group, most patients received conservative (n = 12) or minimally invasive (n = 9) treatment, whereas in the retrospective group all patients (n = 21) underwent open surgery. The nephrectomy rate was higher in the retrospective group. There were no statistically significant differences between the groups in terms of complication rates or length of hospital stay.
Conclusion. Conservative management is the preferred approach for blunt renal trauma with collecting system rupture. In patients who develop a urinoma, ureteral stenting or percutaneous nephrostomy should be performed.
Introduction. Stress urinary incontinence (SUI) is a common condition that can significantly impair women’s quality of life. Despite the proven efficacy of sling procedures, preoperative fears among patients remain an understudied topic, although such fears may affect treatment outcomes and patient satisfaction.
Objective. To investigate preoperative fears among women with SUI and identify factors associated with these concerns.
Materials & methods. The study included 720 women diagnosed with SUI who were scheduled to undergo sling surgery. Preoperative fears were assessed using a custom-developed questionnaire, along with the Hospital Anxiety and Depression Scale (HADS).
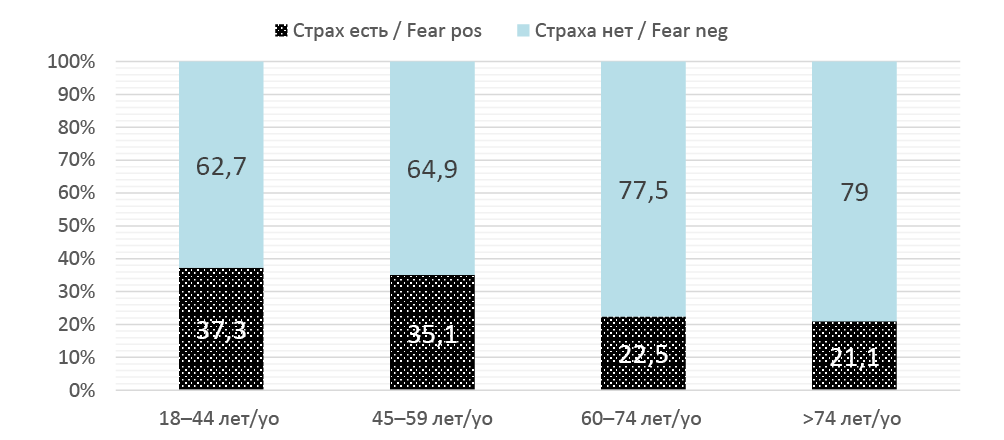
Results. Preoperative fears were reported by 77% of women with SUI. The most frequently reported concerns were persistent urinary leakage requiring continued use of pads (45.1%), complications related to the implant (30.4%), and anesthesia-related fears (25.8%). Women with preoperative fears were significantly more likely to be married (71.0% vs. 62.3%; p = 0.039) and to have undergone previous pelvic reconstructive surgery (45.8% vs. 36.4%; p = 0.037). Higher preoperative anxiety and depression levels on the HADS were associated with a greater number of fears. Fear of implant-related complications was more prevalent among women under 60, with higher education, employed, and residing in urban areas. Fear of anesthesia was more common in employed and previously non-operated women. Fear of persistent symptoms was more frequent among married women and those with a history of reconstructive surgery. Multivariate logistic regression identified marital status, presence of depression, and place of residence as independent predictors of preoperative fears.
Conclusion. Identifying and understanding the nature of preoperative fears in women with SUI may help optimize preoperative counseling and psychological preparation, potentially improving postoperative outcomes.
REVIEWS ARTICLE
Introduction. Vesicourethral anastomotic stricture is a common and clinically significant complication of radical prostatectomy, leading to infravesical obstruction and substantial impairment of quality of life. Despite the availability of endoscopic, stenting, and reconstructive surgical options, recurrence rates remain high, and the optimal management strategy continues to be debated. A comprehensive evaluation of the effectiveness and safety of current treatment approaches is therefore warranted.
Objective. To evaluate and compare the outcomes of different treatment modalities for vesicourethral anastomotic (VUA) strictures following radical prostatectomy (PPE strictures), focusing on anastomotic patency, recurrence, stress urinary incontinence, and quality of life.
Materials & methods. A systematic review and meta-analysis was conducted in accordance with PRISMA guidelines. Medline/PubMed, Embase, and Cochrane Library were searched through January 2025 for original studies including ≥5 patients with PPE-related VUA strictures treated with endoscopic, stenting, or open reconstructive approaches. Primary outcomes included effectiveness (patency), recurrence rates, complications, incontinence, and need for reintervention. Two reviewers independently screened studies, extracted data, and assessed risk of bias (ROBINS-I). The quality of evidence was rated using GRADE.
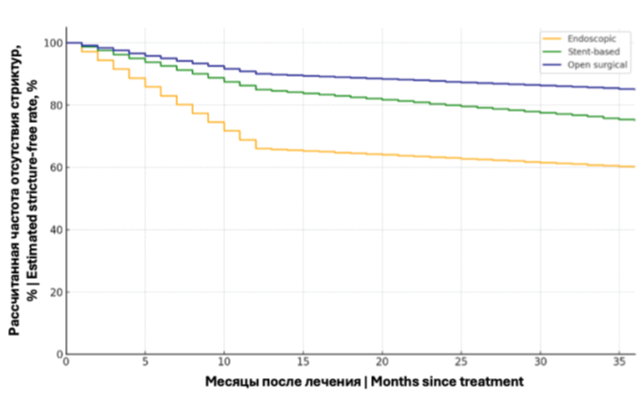
Results. A total of 24 studies (n = 745 patients) were included, primarily retrospective case series. Endoscopic approaches yielded an initial success rate of 55% (95% CI 40 – 70%), increasing to 91% with repeat procedures. Recurrence rates reached 40% within 1 – 2 years. De novo stress incontinence was rare (≤ 5%). Temporary urethral stents (Memokath®️, Allium®️) showed patency rates up to 93%, with migration in 7% and incontinence in ≤ 10% of patients. Open reconstructive techniques, including buccal mucosa grafts, achieved success rates of 73 – 85%, but were associated with new-onset incontinence in 40 – 75% of cases. Radiation history significantly reduced treatment success (OR 0.20; 95% CI 0.05 – 0.80).
Conclusion. Endoscopic procedures are optimal as first-line treatment due to minimal invasiveness and preservation of continence but have high recurrence risk. Temporary stents are a viable intermediate option after failed endoscopy. Open reconstruction provides the most definitive outcomes in complex cases but is burdened by a high incontinence risk. Treatment decisions should be individualized, considering prior radiation, stricture severity, and continence preservation.
Introduction. Prostate biopsy remains the definitive standard for confirming malignancy in the prostate. However, a negative initial biopsy does not rule out the presence of prostate cancer (PCa) during subsequent follow-up. This review provides an overview of current repeat biopsy techniques and assesses their diagnostic accuracy for clinically significant PCa (csPCa).
Objective. To study various methods of repeated biopsy and evaluate the results of diagnosis of csPCa.
Materials & Methods. A review of PubMed, eLibrary electronic databases was conducted from 2000 to 2024 to identify all relevant studies. The electronic search was limited to Russian and English, and the keywords used were: repeat prostate biopsy, clinically significant prostate cancer, fusion biopsy.
Results. Currently, the following techniques can be used to perform a repeat prostate biopsy: saturation biopsy, micro-ultrasound, histoscanning and fusion biopsy. Saturation biopsy is associated with an increase in the number of complications, histoscanning has not shown high efficiency, micro-ultrasound is not so common and is limited by the number of studies. The advantage of diagnosing csPCa in patients with a previous negative histological conclusion is currently behind fusion biopsy. One of the advantages is the ability to choose one of three execution techniques: fusion, cognitive and in bore.
Conclusions. Fusion technique shows the best results of the effectiveness of the diagnosis of csPCa with repeated biopsy. According to the literature, various methods of performing fusion biopsies are comparable to each other.
Introduction. Prostate cancer (PCa) is one of the most common malignancies among men, making the search for new methods of its early detection highly relevant. Existing diagnostic approaches, such as the determination of prostate-specific antigen (PSA) levels, have limited specificity and sensitivity, highlighting the need for more accurate and non-invasive diagnostic methods.
Objecive. To analyze recent studies focused on the use of gas chromatography coupled with mass spectrometry (GC–MS) for the detection of urinary volatile organic compounds (VOCs) as potential PCa biomarkers, as well as to evaluate the prospects for the implementation of this method in clinical practice.
Materials & Methods. The review includes an analysis of scientific publications available in the PubMed, Medscape, and eLibrary databases for the period from 2019 to 2024. The focus was placed on studies devoted to urine metabolomic profiling using GC–MS and investigations of metabolic pathway alterations in prostate cancer cells.
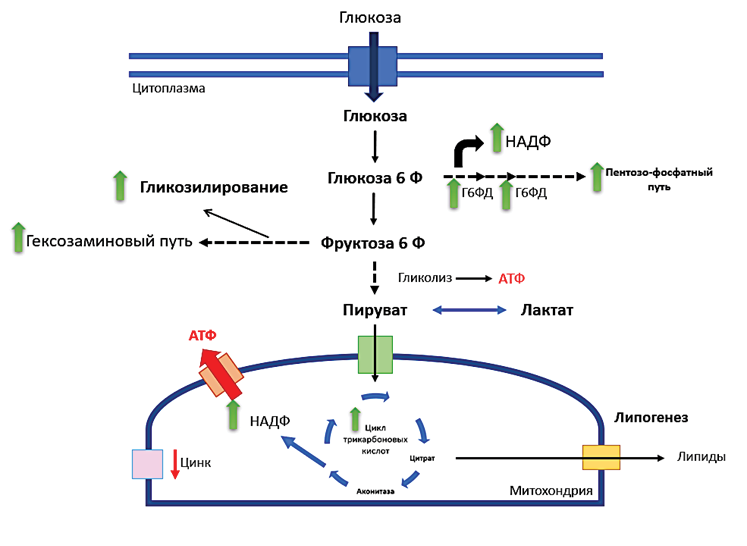
Results. The results of the reviewed studies demonstrate that GC–MS enables the identification of specific VOCs associated with tumor transformation of prostate cells. This method shows high diagnostic accuracy, exceeding traditional approaches such as PSA testing. Metabolites such as sarcosine, acylcarnitine, and arachidonoilamine have been identified as demonstrating high sensitivity and specificity in the diagnosis of PCa. Alterations in carbohydrate and lipid metabolism, as well as activation of the pentose phosphate pathway, were also observed in PCa cells.
Conclusion. The use of GC-MS for VOC analysis in urine is a promising method for diagnosing prostate cancer, offering high accuracy and non-invasiveness. However, implementing this method into clinical practice requires addressing several technical and methodological issues, including standardizing protocols and reducing equipment costs. Further development of metabolomics and refinement of analytical methods could significantly improve early PCa diagnosis, positively impacting prognosis and quality of life for patients.
CLINICAL CASES

Introduction. A rare but serious side effect of pelvic radiation therapy is radiation cystitis, which is characterized by persistent hematuria brought on by gradual ischaemic damage to the bladder mucosa. Bowel irrigation, intravesical therapy, and coagulation methods are examples of conventional treatments that frequently only offer short-term respite without addressing the underlying disease. By improving oxygen delivery to hypoxic areas, hyperbaric oxygen therapy (HBOT) has become a viable substitute that encourages angiogenesis and tissue repair.
Case Presentation. We describe a case of a 77-year-old man who had persistent gross hematuria lasting for two weeks and had a history of prostate cancer diagnosed in 2016, for which he received radiotherapy, with the last session administered in 2018. A flexible cystoscopy showed gradual bleeding and spotty bladder irritation. Laboratoty tests revealed anemia with hemoglobin 9.6 g/dL without renal impairment or coagulopathy. HBOT was started since the hematuria continued even after bladder irrigation. After ten HBOT sessions, the patient's hemorrhage was completely resolved. He had mild adverse effects, such as brief nausea and vomiting, which were treated with medication. The long-term effectiveness of HBOT was demonstrated by follow-up visits, which verified that there was no recurrence of hematuria.
Conclusion. This case highlights the value of HBOT as a non-invasive and safe treatment for refractory hemorrhagic cystitis, a complication of radiotherapy. For individuals who fail to respond to conventional treatments, HBOT presents a viable alternative because it treats the underlying ischaemic damage rather than just treating the symptoms. Further research is required to develop standardized treatment procedures and assess long-term results.
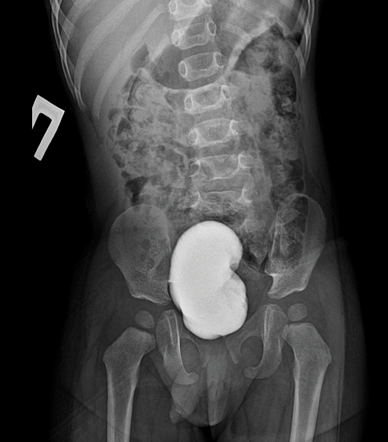
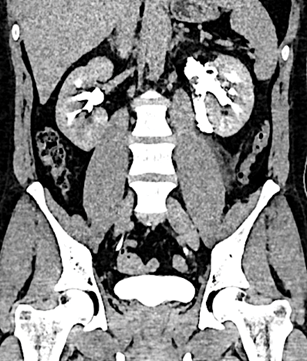
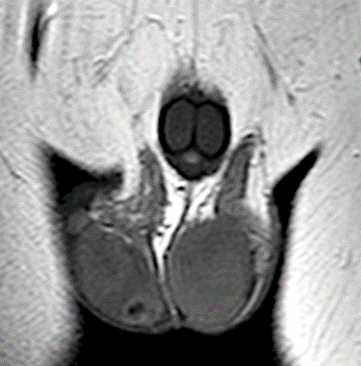
Inflammatory myofibroblastic tumor (IMT) is a rare neoplasm characterized by proliferation of spindle‑shaped cells with prominent inflammatory cell infiltration. IMT is also referred to as an inflammatory pseudotumor or pseudosarcomatous myofibroblastic tumor. Although it accounts for less than 1% of all bladder tumors, the bladder is the most frequent site of IMT within the genitourinary tract. In this report, we present the case of patient M., a 1‑year‑7‑month‑old child with a 2‑month history of dysuria and painful voiding. Following a diagnostic work‑up, including ultrasound, voiding cystography, abdominal and pelvic CT, cystourethroscopy, and pelvic MRI, the child underwent surgical excision (enucleation) of the mass with negative margins. Histopathological examination confirmed the diagnosis of IMT. During 2 years of follow‑up with ultrasound, CT, and MRI, no evidence of local recurrence was detected, which is consistent with published data indicating low recurrence rates after organ‑sparing surgical management without adjuvant chemotherapy.

Skin metastases are rare localization of secondary foci. More rarely, metastases are found in the skin of the head and neck. The article describes a clinical case of identifying two primary lesions in the buccal and submandibular region in a 61-year-old patient with no history of cancer. The examination data showed a hypervascular structure of the lesions, which suggested a diagnosis of vascular malformation. However, histological examination revealed metastases of clear cell renal cell carcinoma to the skin. Further examination revealed a tumor in the left kidney and secondary lesions in both lungs. The described clinical case encourages dermatologists and maxillofacial surgeons to be wary of patients with isolated skin lesions in order not to miss atypical metastases of a renal tumor.
Intratesticular cysts have recently become a common finding in clinical practice. According to research data, such formations are detected in 8.0 – 9.8% of men. Simple intratesticular cysts do not have malignant potential and do not require monitoring or treatment. However, it is crucial to differentiate them from cystic neoplasms, which may conceal malignant processes. This article presents a clinical case of a 30-year-old patient in whom ultrasonography revealed a cystic formation in the right testis with a minimal solid component measuring 7.1 × 6.9 × 8.5 mm. Initially, active surveillance with regular ultrasound monitoring was chosen. However, progressive enlargement of the lesion required surgical intervention. Given the small size of the tumor, an attempt was made at testis-sparing surgery. However, intraoperative morphological examination using frozen sections revealed the malignant nature of the lesion, leading to the performance of a radical inguinal orchiectomy. The final histological examination confirmed the diagnosis of embryonal carcinoma. This clinical case demonstrates an atypical manifestation of embryonal testicular carcinoma in the form of a predominantly cystic lesion with a minimal solid component. The presented case complements existing data on the ultrasound characteristics of embryonal carcinoma and highlights the importance of careful active surveillance even for small cystic formations in testis.
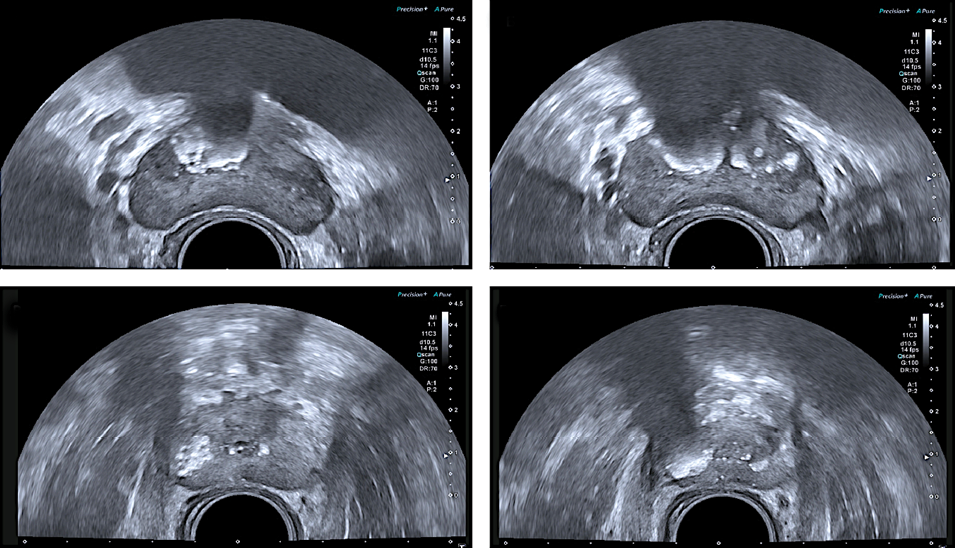
The reported prevalence of prostatic calculi / stones ranges from 7% to 99% and depends on patient age. Prostatic calculi are found in 9% of men aged 18 – 29 years, in 32.3% of those aged 50 – 59 years, and in 66.7% of those aged 70 – 79 years. Prostatic calculi associated with benign prostatic hyperplasia (BPH) are often asymptomatic and are usually detected incidentally during surgical treatment of BPH. Large or multiple calculi, as well as stones associated with chronic prostatic inflammation, may cause nonspecific lower urinary tract symptoms (LUTS). In addition, patients with prostatic calculi may present with hematuria, post‑micturition dribbling, urinary incontinence, and chronic pelvic pain syndrome. Prostatic calculi occurring in the setting of chronic inflammation of the gland can serve as a nidus for bacterial colonization and may promote the selection of microorganisms resistant to antimicrobial therapy. Asymptomatic calculi generally do not require specific treatment and are most often removed incidentally during surgery for prostate cancer. In symptomatic cases, the efficacy of conservative treatment, particularly antibiotic therapy, is limited because the stones themselves represent a persistent source of infection. Therefore, in such patients, the preferred management option, in combination with antibacterial therapy, is endoscopic removal. In this paper, we present our clinical cases in patients with multiple symptomatic and asymptomatic prostatic calculi and provide a review of the relevant literature.








































