




Contents
Scroll to:
https://doi.org/10.21886/2308-6424-2023-11-1-159-164
Scroll to:
Urethral doubling is a rare congenital malformation of the lower urinary tract. A little more than 200 cases of various forms of this defect have been described in the literature worldwide. We present a rare clinical case of duplication of the urethra in combination with the megaureter of the only functioning kidney. In this patient, we encountered a previously undescribed anomaly within the generally accepted classification of the kidney collecting system in combination with a true diverticulum of the bladder and a descending orthotopic ureterocele.
Dutov V.V., Romanov D.V. Urethral doubling in children and adolescents. Urology Herald. 2023;11(1):159-164. (In Russ.) https://doi.org/10.21886/2308-6424-2023-11-1-159-164
Urethral doubling is a rare congenital malformation of the lower urinary tract. In the world literature, slightly over 200 cases of various forms of this malformation were described, which probably describe various embryological defects [1–3]. Despite the many existing theories of the origin of this anomaly, there is no unified interpretation of its development.
Five patients with various forms of urethral doubling were under observation from 2004 to 2017. The patients ranged in age from 5 to 18 years old. The main complaint of all patients or their parents was a cosmetic defect of the penis in the form of two external urethral foramina of different localisations.
The study aimed to present a rare clinical case of urethral doubling combined with a megaureter of a single functioning kidney, true bladder diverticulum, and a descending orthotopic ureterocele.
Patient K. 18 years old. Urination in the doubled stream since birth. Tensive pains in the right lumbar region have appeared intermittently since the age of 14.
A volumetric mass about 10 cm in size, limitedly mobile and moderately painful was palpated in the right abdomen. The external orifice of the urethra was located at the apex of the glans penis. An additional external orifice of the urethra was located in the area of the penile frenulum along the median line (Fig. 1).
Lumbar-iliac dystopia of the right kidney was revealed by ultrasound examination. The pelvis was extrarenal on the anterior surface. The kidney collecting system was dilated (Fig. 2A). The coatings of the descending ureterocele were on the left side (Fig. 2B).
Excretory urography (exposure 85 minutes): no contrast agent release by the left kidney (Fig. 3). Left-sided refluxing megaureter revealed by cystography (Fig. 4). Ascending urethrography revealed urethral doubling (Fig. 5). Renography, dynamic nephroscintigraphy: single functioning right kidney, renographic curve of hydronephrotic type (Fig. 6).
Multislice computed tomography: posterior bladder wall diverticulum. Filled bladder: descending ureterocele coating. The bladder was emptied. The ureterocele coatings were not descending. Multiple congenital combined anomalies of the urinary system organs (Fig. 7).
Diagnosis – "Multiple congenital combined anomalies of the urinary system organs. Single functioning lumbosacral iliac dystopian right kidney. Obstruction of the right ureteropelvic junction. Uninfected right-sided hydronephrosis. Hypoplasia of the left kidney. Left-sided giant refluxing megaureter. Orthotopic descending ureterocele on the left. True bladder diverticulum. Urethral doubling".
Surgical treatment — right-sided ureteropyeloneostomy was performed (Figs. 8, 9).

Figure 1. The external urethral opening is located at the top of the glans penis. The additional external urethral opening is visualized near the penile frenulum along the midline
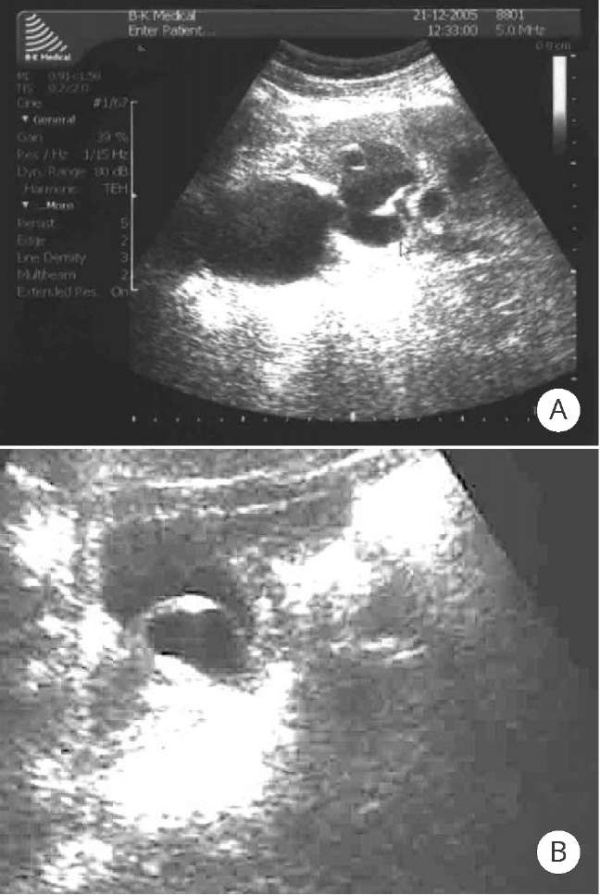
Figure 2. Ultrasound scans: A — iliac dystopia of the kidney; the pelvis is extrarenal on the anterior surface, the collecting system of the kidney is dilated; B — ureterocele wall penetration into the lumen of the posterior urethra

Figure 3. Contrast-enhanced urography scan: lumboiliac dystopia of the right kidney, ureterohydronephrosis

Figure 4. Voiding cystography scan: left-sided refluxing megaureter

Figure 5. Retrograde urethrography scan: urethral doubling
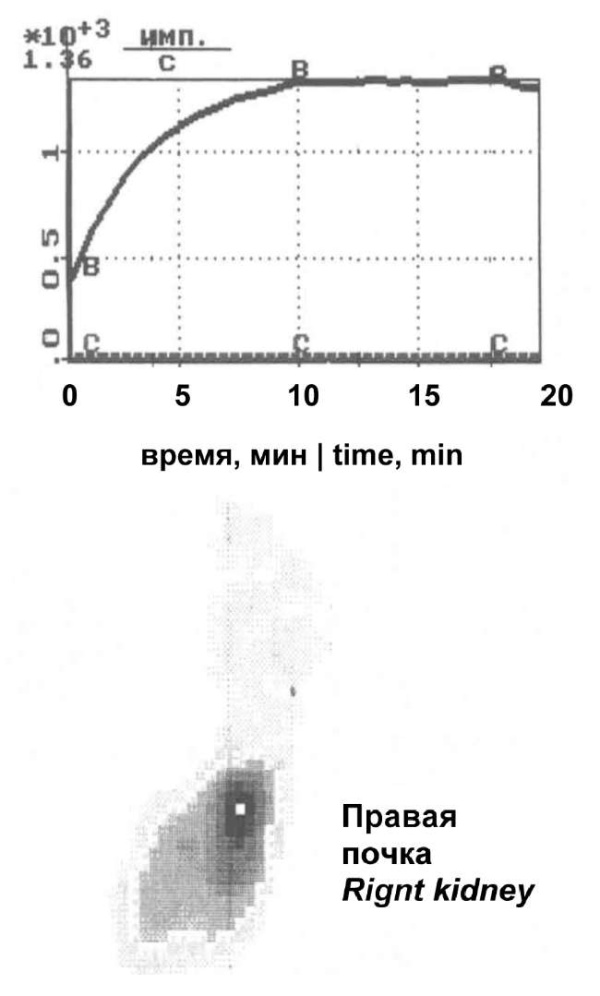
Figure 6. Renography, dynamic nephroscintigraphy scans: sole functioning right kidney; renographic curve according to hydronephrotic type
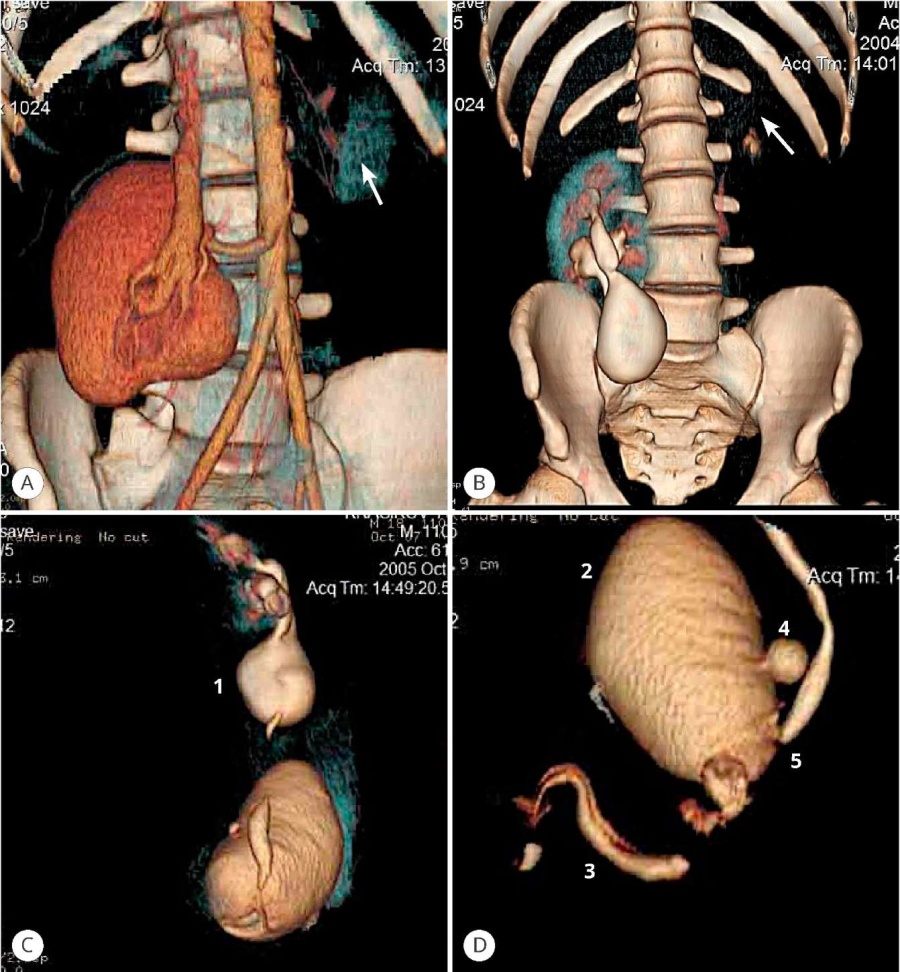
Figure 7. CT scans: rudimentary left kidney (arrow), dystopia of the right kidney; anomaly of the collecting system: megaureter (1), bladder (2), double urethra (3), posterior wall diverticulum (4), ureter (5)
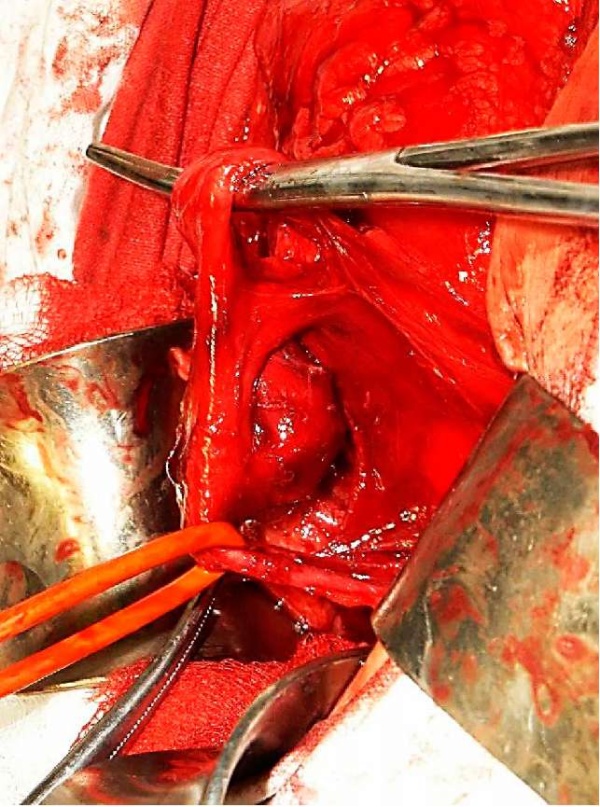
Figure 8. Surgery stage: right-sided ureteropyeloneostomy

Figure 9. After surgery. Antegrade pyeloureterography scan.
The Y-shaped variant of urethral doubling is the most common (Fig. 10) [4][5]. In this variant, the anterior and posterior urethra usually retain their functionality and sphincter mechanism. The dorsal (orthotopic) urethra is usually weaker developed. Some authors refer to a subtype of urethral doubling as a congenital urethro-cutaneous fistula. Y-type urethral doubling is often combined with other serious congenital anomalies, such as nonperforated anus, prune belly syndrome, bladder extrophy, cloaca formation, malformations of the spine, intestine, esophago-tracheal fistula, and various types of genitourinary organ anomalies: renal dysplasia, hypoplasia, and aplasia, hydronephrosis, polycystic kidneys, upper urinary tract doubling, vesicoureteral reflux, cryptorchidism, and hypospadias [3][6]. Urethral stenosis may also be detected in some patients.
The clinical manifestations are highly variable. The patient may have signs of upper and lower urinary tract obstruction, the progression of which leads to chronic renal failure [7].
Knowledge of possible variants of urethral doublings [4], as well as the most frequent variants of combined anomalies, is an important point in planning the examination and determining surgical correction tactics.
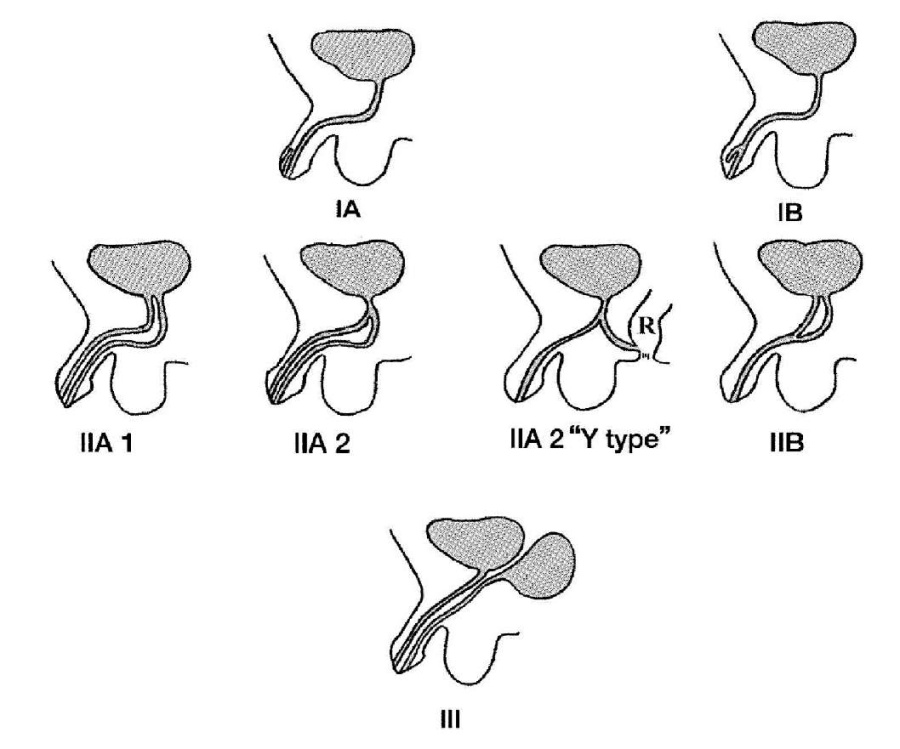
Figure 10. Effman classification of urethral doubling in men [4]
Surgical treatment of urethral doubling depends on the anatomic form of the doubling and the clinical manifestations. Patients with minimal clinical manifestations do not require surgical correction. Correction of urethral doublings should be aimed at eliminating cosmetic defects, doubling of the urine stream, and elimination of infravesical obstruction, and urinary incontinence.
1. Erdil H. Congenital anomalies of the kidneys in family members. Ann Saudi Med. 2003;23(3-4):231-2. DOI: 10.5144/0256-4947.2003.231
2. Bae KS, Jeon SH, Lee SJ, Lee CH, Chang SG, Lim JW, Kim JI. Complete duplication of bladder and urethra in coronal plane with no other anomalies: case report with review of the literature. Urology. 2005;65(2):388. DOI: 10.1016/j.urology.2004.08.043
3. Sindjic S, Perovic SV, Djinovic RP. Complex case of urethral duplication with megalourethra. Urology. 2009;74(4):903-5. DOI: 10.1016/j.urology.2008.12.040
4. Effmann EL, Lebowitz RL, Colodny AH. Duplication of the urethra. Radiology. 1976;119(1):179-85. DOI: 10.1148/119.1.179
5. Kagantsov I.M., Sannikov I.A., Golovin A.V., Svarich V.G. Rare case of urethral duplication in the boy. Urology Herald. 2020;8(2):107-112. (In Russian). DOI: 10.21886/2308-6424-2020-8-2-107-112
6. Bar-Moshé O, Oboy G, Timmermans C, Vandendris M. Megalourethra and abnormalities of the cavernous bodies: cause of erectile dysfunction. Eur Urol. 1995;27(3):249-51. DOI: 10.1159/000475171
7. Podesta ML, Medel R, Castera R, Ruarte AC. Urethral duplication in children: surgical treatment and results. J Urol. 1998;160(5):1830-3. DOI: 10.1016/s0022-5347(01)62427-3
Valery V. Dutov — M.D., Dr.Sc.(Med), Full Prof.; Head, Dept. of Urology, Leading Researcher,
Moscow
Dmitry V. Romanov — M.D., Cand.Sc.(Med); Assist.Prof., Dept. of Urology, Senior Researcher,
Moscow
Dutov V.V., Romanov D.V. Urethral doubling in children and adolescents. Urology Herald. 2023;11(1):159-164. (In Russ.) https://doi.org/10.21886/2308-6424-2023-11-1-159-164

Editor-in-Chief
 Vladimir P. Glukhov
Vladimir P. Glukhov
29 Nakhichevanskiy Ln., Rostov-on-Don, 344022, Russian Federation, Rostov State Medical University, Department of Urology and Pediatric Urology
Phone: +7 (863) 201-44-48
e-mail: urovest@mail.ru






































