




Contents
Scroll to:
https://doi.org/10.21886/2308-6424-2023-11-1-100-107
Scroll to:
Introduction. Currently, several virtual reality (VR) simulators have been described for the upper urinary tract stone surgery skill development, including retrograde or antegrade nephroscopy. However, their high cost and the lack of a detailed reconstruction of the intraluminal pelvicalyceal system (PCS) appearance limit their implementation into educational process and clinical practice.
Objectives. To develop the approach for VR-reconstruction of the intraluminal appearance of the PCS via head mounted device (HMD), as well as estimate its usefulness for novices to improve spatial orientation during retrograde flexible nephroscopy.
Materials & methods. Five residents without experience in self-performing retrograde flexible nephroscopy participated in a 7-day training course on the VR simulator developed, during which each novice studied six variants of the PCS. For the procedure simulation, a silicone kidney model was created with the stone placed in the calyx which was selected randomly in each case. Before and after VR-course, each resident assisted the experienced urologist during simulated retrograde nephroscopy to find the stone placed according to random selection. The nephroscopy time and the number of errors in stone-finding during retrograde flexible nephroscopy were analysed.
Results. There was a statistically significant decrease in nephroscopy time (on avg by 17.6 minutes, p = 0.043) and errors to find targeted calyx, which was observed once after the training one resident only.
Conclusion. The described VR simulator does not require significant time, technical and financial costs, and is available for wide implementation in the training of young specialists.
Talyshinskii A.E., Guliev B.G., Mishvelov A.E., Agagyulov M.U., Andriyanov A.A. Virtual reality simulator for developing spatial skills during retrograde intrarenal pyeloscopy. Urology Herald. 2023;11(1):100-107. (In Russ.) https://doi.org/10.21886/2308-6424-2023-11-1-100-107
Urolithiasis is a common disease that occurs in 10% of the population in the Russian Federation [1]. Despite the determination of risk factors and the development of preventive methods, the treatment of most patients require surgical interventions, which emphasises the importance of urologists mastering the existing surgical aids. Currently, open surgery for upper urinary tract stones is almost completely replaced by minimally invasive interventions such as percutaneous nephrolithotripsy (PNL) and retrograde intrarenal surgery (RIRS), each with distinct steps, the correct and safe performance of each of which influences the success of the entire operation [2]. There are several challenges in the process of mastering endourological surgery by young specialists, such as the long learning curve and the need to ensure patient safety [3]. Virtual reality (VR) is a promising direction in the visualisation and simulation of surgical stages, which allows it to be used to address the limitations mentioned above [4]. However, the available developments are too expensive, they are based on the use of a template pelvicalyceal system (PCS) and are of little use for practicing nephroscopy in an environment with full virtual immersion, which is especially important due to the lack of direct visualization of the operating field in endoscopic interventions [5].
The study aimed to describe the technique of VR-guided construction of the internal view of the kidney pyelocaliceal system using a specialized head-mounted device (HMD) and to test it for training residents in spatial orientation during retrograde pyelocalicoscopy.
At the beginning of the study, CT urograms of six patients with different variants of the renal cavity system were selected. Of these, four corresponded to Sampaio types of renal cavity system, and in two patients, the Horseshoe and Duplex Kidney PCSs were selected. In all cases, a three-dimensional reconstruction of the PCS was performed and saved in stereolithography (STL) format using RadiAnt DICOM Viewer. Then, the Blender open-source software was used to smooth the obtained shapes and then transfer the files to a smartphone. This process took about 2 to 3 minutes on average. This work was based on the InsKid application, developed using the C Sharp (C#) programming language for Android-based smartphones [6]. After opening the STL file with the kidney cavity system, it can be run in two modes (2D and VR). In the first case, the internal and external three-dimensional (3D) reconstruction is displayed in the left and right windows of the smartphone, respectively. The red triangle in the right window reflects the actual position of the user and the direction of view (Fig. 1).
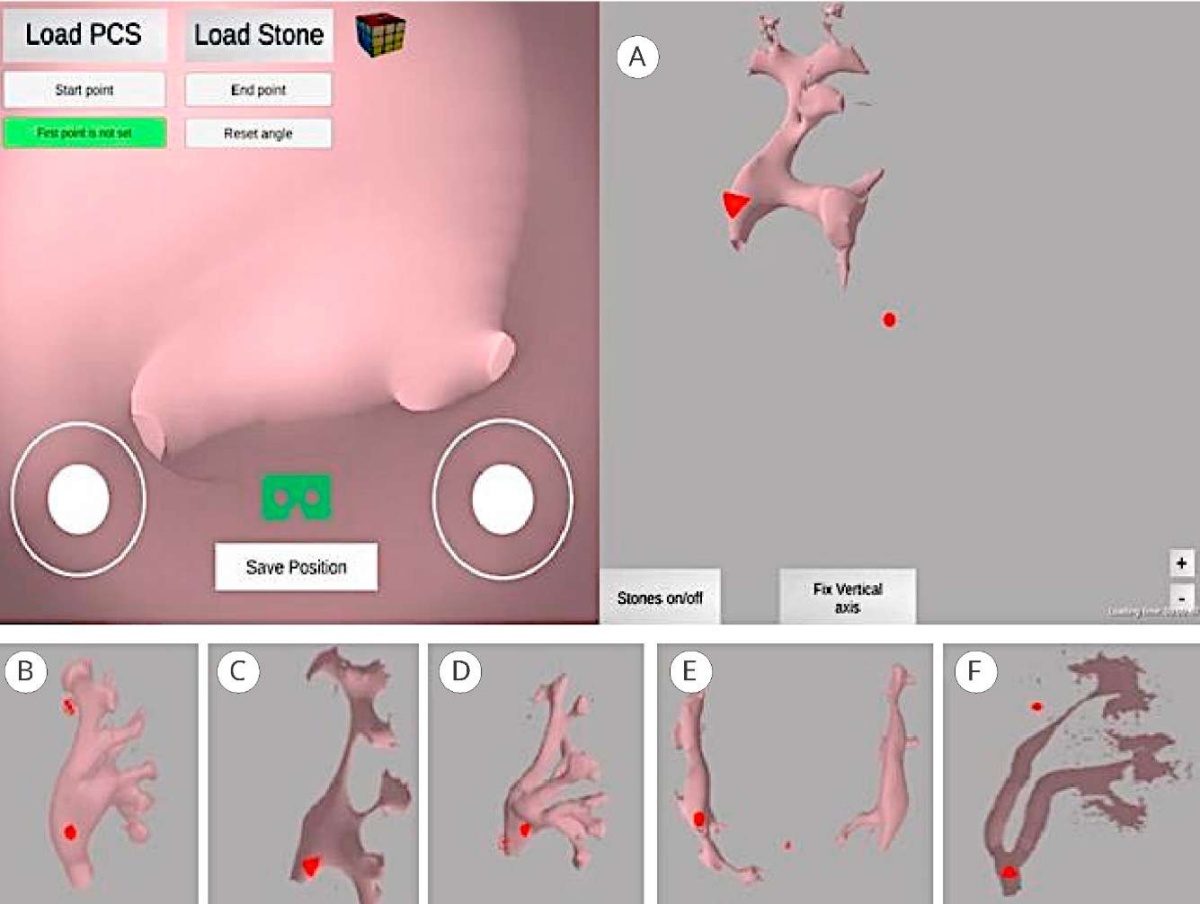
Figure 1. 2D view of the InsKid application from the smartphone screen; internal and external appearance of the renal pyelocaliceal system, according to the Sampaio classification: A — type IA; B — type IB; C — type IIA; D — type IIB; E — horseshoe kidney; F — upper urinary tract of the left incomplete duplication kidney
In VR mode, the user sees the external reconstruction of the renal PCS, and then, they can enter it anywhere and move around inside. It was guided using a PS4 controller connected to the phone via Bluetooth. In 2D mode, the right and left joysticks are responsible for moving along the plane or changing the direction of the view. In VR mode, the left joystick is responsible for moving in the plane and the gaze direction corresponds to head movements. In both cases, one can visualize kidney stones by saving them in the STL format and loading them into the application. It is also possible to manually create different virtual shapes that simulate kidney stones. Thus, in the present work, a sphere corresponding to the stone model was generated using the Blender 3D CG® software (Blender Foundation, Amsterdam, the Netherlands). To run smoothly, the application was run on a Samsung A51 smartphone (equipped with an Exynos 9611 processor, 4 GB of memory, and a Mali-G72 MP3 graphics accelerator), which was placed in the VR Box 3D HMD (Fig. 2).
For evaluation, five residents with no experience performing flexible pyeloscopy were included in the training. Each of them was shown on the computer an external 3D-reconstruction of the kidney with the numbering of small calyces, on the basis of which a silicone model of the kidney was prepared. The kidney cavity system was specifically chosen without stones to randomly identify the small calyx containing the nodule.

Figure 2. The necessary equipment for the VR simulator
Next, all apprentices took turns going to the operating room to assist an experienced urologist in stone retrieval during retrograde flexible pyeloscopy with a LithoVue™ endoscope (Boston Scientific Corp., San Jose, CA, USA), namely, guiding its movements to find the stone (Fig. 3).
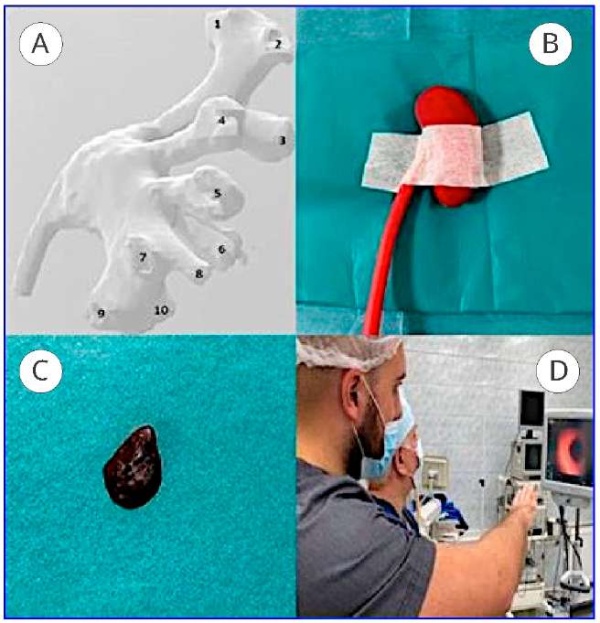
Figure 3. 3D reconstruction of the renal pelvicalyceal system with calyceal numeration (A); B – silicon kidney model for retrograde flexible nephroscopy (B); kidney stone model (C); the resident navigates the urologist to find the stone (D)
At this stage, the time of the procedure and the number of mistakenly examined bowls were determined. The next stage was a 7-day training course; the residents were introduced to the principles of application performance. Each resident examined six of the cavities described above in VR mode for 15 minutes each day.
After a week of VR training, each resident virtually examined the PCS of a silicone kidney model for 10 minutes. In each case, a small calyx was also randomly determined, wherein the stone would be located. The virtual sphere was placed in the VR image by the researcher; after that, the phone was placed in the glasses for a direct study by the residents themselves (Fig. 4). Then, each participant again went to the operating room to navigate the movements of the urologist during retrograde flexible pyeloscopy, and the stone was placed in the small cup according to the result of randomization without notifying anyone in the operating room.
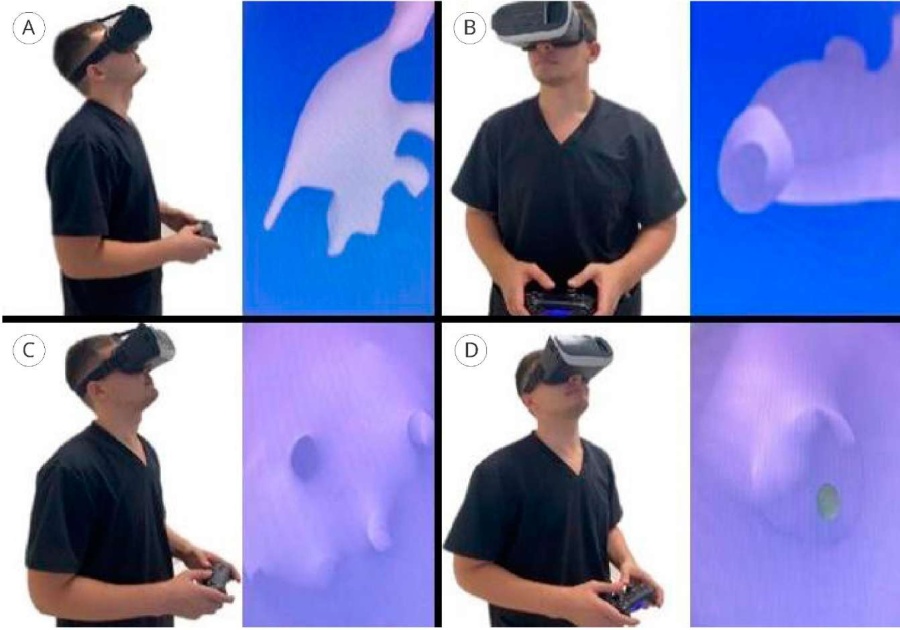
Figure 4. The resident investigates the virtual appearance of the kidney cavity before retrograde flexible nephroscopy: A — external examination of the cavity; B — visualization of the ureteral lumen for penetration into the cavity; C — examination of the lower and middle calyceal groups; D — detection of a virtual stone in the upper calyx
The nephroscopy time and the number of small calyces mistaken for containing a stone were measured similarly to the pre-training evaluation. The described results were compared before and after the VR course.
Statistical analysis. The SPSS software version 26.0 (SPSS: An IBM Company, IBM SPSS Corp., Armonk, NY, USA) was used for statistical analysis. Continuous data were presented as the mean and range between minimum and maximum values due to a small sampling size. Results before and after VR training were compared using the Wilcoxon test. A significant difference was considered at p < 0.05.
The total cost of the simulator was 27$ (joystick + HMD, not including the cost of the smartphone). The preparation time of the STL model of a printed kidney and six cavities for training was 17 minutes.
The frame frequency at the start of the application in VR mode on the described smartphone was 79 frames per second, which indicates the suitability of medium-class devices for the implementation of the described training. The results of the testing are presented in the Table.
Table. Results of assisting residents during retrograde flexible pyeloscopy
|
Variables |
Resident's number |
Mean (interval) |
p |
|||||
|
1 |
2 |
3 |
4 |
5 |
||||
|
Nephroscopy time (sec) |
Before the study |
29 |
23 |
18 |
52 |
21 |
28.6 (18 – 52) |
0.043 |
|
After the study |
11 |
8 |
10 |
15 |
11 |
11 (8 – 15) |
||
|
Mistakes (n) |
Before the study |
3 |
1 |
2 |
4 |
3 |
2.6 (1 – 4) |
0.039 |
|
After the study |
0 |
0 |
0 |
1 |
0 |
0.2 (0 – 1) |
||
There was a statistically significant improvement in the parameters studied: the average duration of pyeloscopy decreased by 17.6 minutes (p = 0.043); after training, the erroneous detection of the target calyx was observed once only in one resident.
The training of surgeons is now increasingly expanding beyond the operating room, allowing for a significant portion of the learning curve to be passed without direct influence on the patient. Simulators contributing to this trend are divided into biological, non-biological, and virtual reality-based simulators according to the production principle [7]. Although physical simulators provide haptic feedback, their usefulness in training is similar to that of VR simulators [8]. The latter allow the use of various anatomical virtual models without the need to manufacture them and do not depend on the use of endourological instruments, prone to breakage in the initial stages of the mastering of certain manipulations by specialists [9].
Several VR-based solutions for skill development and preoperative planning for minimally invasive treatment of upper urinary tract stones were described in the literature. UroMentorTM (Simbionix, Cleveland, OH, USA) is a simulator that simulates rigid or flexible cysto/uretero/pyeloscopy with the ability to perform lithotripsy and fragment extraction [10]. The PERC Mentor™ simulator (Simbionix, Cleveland, OH, USA) is a simulator of antegrade treatment of cavitary kidney stones without the use of specialized glasses with image projection on a 2D monitor [11]. Breakthrough is the development of K181 PCNL & Kidney Access Array (Marion Surgical Inc., Buffalo, NY, USA). It is a simulator of percutaneous surgery of renal cavitary stones using a VR HMD and the ability to download CT images from a particular patient [12]. Finally, Parkhomenko et al. described a technique of VR planning of renal cavity puncture to improve PNL results, allowing loading of renal structures and neighbouring organs into VR glasses [13].
Mastering the skills to perform endourological interventions for urolithiasis includes not only the achievement of competence in the initial stages of surgery, but also the ability to navigate in confined spaces such as the renal cavity. Despite the relatively wide range of available VR simulators, only two of them use VR glasses. Only one of them allows virtual nephroscopy using patient-specific CT images (Marion Surgical K181). In addition, the cost is also a factor hindering the introduction of VR simulators into clinical practice and into the training process of residents and students. The simulators described above are developed abroad and cost more than $20,000. Parkhomenko et al. developed a more available simulator, which allows specialists to plan the puncture of the kidney cavity by displaying the kidney and adjacent structures in VR glasses, but without the possibility of PCS visualisation from the inside. According to the authors' calculations, the final cost is $1,700 [13]. All this highlights the prospect of the development of virtual reality technology in the Russian Federation. The described VR simulator does not require significant time and financial costs, while allowing the tutors to immerse students in the kidney cavity system in more detail in comparison with the analogs.
The reverse side of the coin is the essence of this kind of technology. According to Moran et al., adding elements of interactive learning to young physicians has a positive effect on their participation and abilities, which is also partially confirmed by the present study [14]. It is not surprising that the modern generation is more familiar with various digital devices and technologies and is more often interested in computer games, including VR.
The present study has certain limitations. First, a small number of residents were included and they were all trained at the same base, which does not allow for conclusions to be drawn about similar usefulness for young professionals in general. At the time of writing the manuscript, 2 additional apprentices (a 5th-year student and a 2nd-year resident from another clinical base) were included. Second, the training was short (7 days) and was conducted in the facilities of the urology department, despite the possibility of such a training even at home. Third, all virtual models were prepared by a colleague and not by the subjects themselves. The spatial orientation skill was analysed, while endourological interventions also require the development of manual skills. Nevertheless, the above-mentioned limitations are beyond the scope of the objectives and will be addressed in future studies.
The described VR simulator does not require significant time, technical, and financial resources and is available for implementation in the training of young specialists.
1. Gadzhiev N, Prosyannikov M, Malkhasyan V, Akopyan G, Somani B, Sivkov A, Apolikhin O, Kaprin A. Urolithiasis prevalence in the Russian Federation: analysis of trends over a 15-year period. World J Urol. 2021;39(10):3939-3944. DOI: 10.1007/s00345-021-03729-y
2. Tzelves L, Türk C, Skolarikos A. European Association of Urology Urolithiasis Guidelines: Where Are We Going? Eur Urol Focus. 2021;7(1):34-38. DOI: 10.1016/j.euf.2020.09.011
3. Quirke K, Aydin A, Brunckhorst O, Bultitude M, Khan MS, Dasgupta P, Sarica K, Ahmed K. Learning Curves in Urolithiasis Surgery: A Systematic Review. J Endourol. 2018;32(11):1008-1020. DOI: 10.1089/end.2018.0425
4. Del Pozo Jiménez G, Rodríguez Monsalve M, Carballido Rodríguez J, Castillón Vela I. Virtual reality and intracorporeal navigation in urology. Arch Esp Urol. 2019;72(8):867-881. (In English, Spanish). PMID: 31579046
5. Igarashi T, Suzuki H, Naya Y. Computer-based endoscopic image-processing technology for endourology and laparoscopic surgery. Int J Urol. 2009;16(6):533-43. DOI: 10.1111/j.1442-2042.2009.02258.x
6. Guliev B, Komyakov B, Talyshinskii A. Interior definition of the calyceal orientation suitable for percutaneous nephrolithotripsy via mobile software. Urolithiasis. 2021;49(5):443-449. DOI: 10.1007/s00240-021-01253-7
7. Gadzhiev N.K., Mishchenko A.A., Britov V.P., Khrenov A.M., Gorelov D.S., Obidnyak V.M., Grigoriev V.E., Semenyakin I.V., Petrov S.B. Creation of a training simulator model for practising puncture of the kidney calyceal system under ultrasound control. Urology Herald. 2021;9(1):22-31. (In Russian). DOI: 10.21886/2308-6424-2021-9-1-22-31
8. Mishra S, Kurien A, Ganpule A, Muthu V, Sabnis R, Desai M. Percutaneous renal access training: content validation comparison between a live porcine and a virtual reality (VR) simulation model. BJU Int. 2010;106(11):1753-6. DOI: 10.1111/j.1464-410X.2010.09753.x
9. Afane JS, Olweny EO, Bercowsky E, Sundaram CP, Dunn MD, Shalhav AL, McDougall EM, Clayman RV. Flexible ureteroscopes: a single center evaluation of the durability and function of the new endoscopes smaller than 9Fr. J Urol. 2000;164(4):1164-8. PMID: 10992358
10. Aloosh M, Couture F, Fahmy N, Elhilali MM, Andonian S. Assessment of urology postgraduate trainees' competencies in flexible ureteroscopic stone extraction. Can Urol Assoc J. 2018;12(2):52-58. DOI: 10.5489/cuaj.4570
11. Zhang Y, Yu CF, Liu JS, Wang G, Zhu H, Na YQ. Training for percutaneous renal access on a virtual reality simulator. Chin Med J (Engl). 2013;126(8):1528-31. PMID: 23595389
12. Sainsbury B, Łącki M, Shahait M, Goldenberg M, Baghdadi A, Cavuoto L, Ren J, Green M, Lee J, Averch TD, Rossa C. Evaluation of a Virtual Reality Percutaneous Nephrolithotomy (PCNL) Surgical Simulator. Front Robot AI. 2020;6:145. DOI: 10.3389/frobt.2019.00145
13. Parkhomenko E, O'Leary M, Safiullah S, Walia S, Owyong M, Lin C, James R, Okhunov Z, Patel RM, Kaler KS, Landman J, Clayman R. Pilot Assessment of Immersive Virtual Reality Renal Models as an Educational and Preoperative Planning Tool for Percutaneous Nephrolithotomy. J Endourol. 2019;33(4):283-288. DOI: 10.1089/end.2018.0626
14. Moran GW, Margolin EJ, Wang CN, DeCastro GJ. Using gamification to increase resident engagement in surgical training: Our experience with a robotic surgery simulation league. Am J Surg. 2022;224(1 Pt B):321-322. DOI: 10.1016/j.amjsurg.2022.01.020
Ali E. Talyshinskiy — M.D.; Deputy CEO for Digital Development in Medicine;
Urologist, Urology Centre with Robot-assisted Surgery,
Moscow
Bakhman G. Guliev — M.D., Dr.Sc.(Med), Full Prof.; Prof., Dept. of Urology,
Head, Urology Centre with Robot-assisted Surgery,
St. Petersburg
Artem Е. Mishvelov — Junior Researcher, Laboratories for the Transfer of Innovative Medical Technologies and Products,
Stavropol
Murad U. Agagyulov — M.D.; Postgrad. Student, Dept. of Urology,
St. Petersburg
Alexander A. Andriyanov — Resident, Dept. of Urology,
St. Petersburg
Talyshinskii A.E., Guliev B.G., Mishvelov A.E., Agagyulov M.U., Andriyanov A.A. Virtual reality simulator for developing spatial skills during retrograde intrarenal pyeloscopy. Urology Herald. 2023;11(1):100-107. (In Russ.) https://doi.org/10.21886/2308-6424-2023-11-1-100-107

Editor-in-Chief
 Vladimir P. Glukhov
Vladimir P. Glukhov
29 Nakhichevanskiy Ln., Rostov-on-Don, 344022, Russian Federation, Rostov State Medical University, Department of Urology and Pediatric Urology
Phone: +7 (863) 201-44-48
e-mail: urovest@mail.ru






































